Deafferentation pain
Misunderstandings and their recognition
in the context of neuropathic pain
Short review
Pathos 2025; 32.3. Online 2025, Oct 30
_________________________________________________________________________________
Guido Orlandini
Medicina del dolore,
Villa Ravenna (Chiavari, Ge)
_________________________________________________________________________________
Summary
The term ‘deafferentation pain’ was introduced in the late 1970s as a synonym for ‘denervation pain’ and has been widely used to generically refer to neuropathic pain, even in situations such as phantom limb pain, atypical facial pain, reflex sympathetic dystrophy and many others, where it was not at all appropriate. In reality, in order to have a clear pathogenetic meaning, the term must refer to neuropathic pain due to a lesion of the spinal or cranial ganglion and/or the dorsal root or the corresponding structure of the cranial nerves.
Riassunto
La dizione “dolore da deafferentazione” è stata introdotta sul finire degli anni Settanta come sinonimo di “dolore da denervazione” ed è stata ampiamente usata per indicare genericamente il dolore neuropatico anche in riferimento a situazioni come il dolore dell’arto fantasma, il dolore facciale atipico, la distrofia simpatica riflessa e molte altre, dove non era assolutamente appropriata. Actually, perché possa avere un chiaro significato patogenetico, la dizione deve riferirsi al dolore neuropatico dovuto a una lesione del ganglio spinale o cranico e/o della radice dorsale o della corrispondente struttura dei nervi cranici.
Key words
Deafferentation pain, phantom limb pain, postherpetic neuralgia
Parole chiave
Dolore da deafferentazione, dolore dell’arto fantasma, nevralgia post-herpetica
Introduction
Even today, neuropathic pain is still often mistakenly considered to be 'deafferentation pain', without a clear reference to a specific type of nerve damage (which would require the definition of particular pathological mechanisms), but rather simply to a 'lack of afferents'.1-5 This imprecise interpretation leads to the erroneous conclusion that phantom limb pain syndrome, phantom tooth syndrome and phantom sinus syndrome are all deafferentation pain, as there is a lack of afferents from the missing limb or tooth. The same applies to pain secondary to peripheral nerve injury. Some even interpret deafferentation pain as '...an umbrella covering all pathologies with or without pain, including neoplastic situations'.6
Literature review
If we search PubMed for the term “deafferentation pain” in the title or abstract, we see that it appears in 303 publications since 1978, almost always generically understood as a lack of afferents resulting from nerve damage at any level, from peripheral to central neurons. The term deafferentation pain as a generic consequence of nerve damage. 7 is casually referred to causalgia, phantom limb pain, brachial plexus avulsion syndrome, post-herpetic neuralgia, reflex sympathetic dystrophy, and amputation. 8-12 .
Considering these different associations, we see that in causalgia (which is due to damage to a large peripheral nerve trunk), axonal neuropathy occurs and the second neuron is not deafferented at all; in phantom limb pain associated with the production of amputation neuroma, the second neuron is not deafferented because afferents from the neuroma reach it; in brachial plexus avulsion syndrome, there are concomitant lesions of the proximal portions of the large peripheral nerve trunks that cause pain from axonal neuropathy and do not involve deafferentation and radicular lesions that can actually cause it; in post-herpetic neuralgia, which is almost always considered deafferentation pain, the pain may be due to lesions in various parts of the peripheral nerve .13 and only when the dorsal root is affected does this type of neuropathic pain actually occur.
The work of Sánchez-Ledesma et al 14 is disconcerting in reference to CRPS-I, where deafferentation pain even affects a situation in which there is no nerve damage. Spinal cord injuries are also classified as deafferentation pain 15-17 and elsewhere we read that atypical facial pain arising following a dental procedure is deafferentation pain, when in fact it should be understood as trigeminal neuropathy, as fortunately reported in other more credible communications.18
Misunderstandings
The first misunderstanding concerns the fact that the concept of “deafferentation” can mean “lack of afferents from...” or “lack of afferents to...”: it is clear that in the first sense, the phantom limb situation involves deafferentation, but if we consider the “lack of afferents to...” and define central neurons as subjects that do not receive afferents, the afferents are there because, even if they do not come from the anatomical structure that is no longer there, they still come from the amputation neuroma, and therefore it is not correct to say that phantom limb pain is caused by deafferentation.
Abandoning the misleading concept of deafferentation as “lack of afferents from...” and accepting that of “lack of afferents to...”, an attempt to rationalize the use of this term derives from Kerr's observation,20 according to which there are three lesions that cause deafferentation: 1) lesion of the dorsal root; 2) lesion of the anterolateral quadrant of the spinal cord; 3) lesion of the thalamus and brainstem. All three of these lesions involve “deafferentation of the upstream neuron,” but while in the first the lesion is peripheral (involving deafferentation of the second neuron), in the other two the lesion is central (involving deafferentation of the thalamus and cerebral cortex, respectively). Let us consider the situation of thalamic deafferentation: in reality, it consists of the elimination of afferents to the reticulothalamic nucleus following damage to the neospinothalamic tract with suppression of the GABAergic inhibition it exerts on the interlaminar nuclei, which, in turn, receive paleospinothalamic afferents. This observation, however, causes further misunderstanding because so-called “central deafferentation” coincides with damage to the central neurons responsible for central pain, leading to the confusing assumption that the latter is also deafferentation.
Another source of confusion and misunderstanding concerns the reported risk of deafferentation pain as a complication of neurolesive procedures. 21 In reality, this complication is possible in the case of trigeminal thermorizotomy if excessive damage is done involving the Aβ fibers and not if only the Aδ and C fibers are involved. In the case of a theoretical peripheral neurotomy (which, in reality, has no clinical indication), what may occur as a complication is neuropathic pain from axonal neuropathy and not from deafferentation. In the case of percutaneous cervical cordotomy, a complication that may occur is central pain if the lesion of the lateral spinothalamic tract is incomplete, involving the neo-spinothalamic tract but sparing the paleo-spinothalamic tract.
Attempt at rationalization
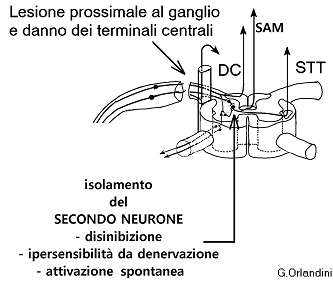
One must agree with Boivie's observation 22 that advises against the use of the term deafferentation pain to indicate central pain, reserving it for pain caused by injury to the first neuron. Even so, however, this does not provide sufficient clarity because if the lesion of the first neuron is distal to the spinal or cranial ganglion, the second neuron continues to receive afferents from the neuroma and is therefore not deafferented. Ultimately, if we really want to attribute a pathogenetic meaning to this term, which was simply coined as a more elegant synonym for ‘denervation’ and is still used today to refer to any pain caused by nerve injury, we can only refer it specifically to the consequences of injury to the first neuron in the spinal or cranial ganglion or in the dorsal root proximal to the ganglion (Figure 1), as a result of which the second neuron is effectively deafferented, according to a concept that I first reported in the first edition of Semeiotica del dolore 23 and reiterated in my subsequent publications 13 and which I must consider tacitly accepted, since it has never been contested.
{kind=link}
According to this theory, damage to the first neuron in the dorsal root ganglion or in the dorsal root proximal to the ganglion or in the corresponding structures of the cranial nerves causes deafferentation pain, which is due to the deprivation of the second neuron of all types of afferents (Aα, Ab, Ad and C). If the lesion involves the ganglion, the entire peripheral neuron is destroyed because the trophic center represented by the pyrenophore fails to function. If it affects the dendrites proximal to the ganglion, the peripheral fibers and the ganglion remain intact, but the central terminals separated from the trophic center degenerate. In either case, the second neuron is disconnected from the first.
Together with the degeneration of the central terminals, nerve damage in the ganglion or proximal to the ganglion leads to disinhibition, denervation hypersensitivity, and spontaneous activation of the second neuron.
Considering the above, the crucial element in the pathogenesis of deafferentation pain is spontaneous epileptiform discharge, first at the medullary level and then, perhaps, also at the thalamic 24 and cortical 25 levels. Another factor to bear in mind is that (as in axonal neuropathic pain) the electrical activity produced in this way in the spinal cord is not only conveyed by the pathways of the anterolateral quadrant of the spinal cord (spinal lemniscus) that conduct normal nociception but, in the absence of activation by the C fibers of the inhibitory interneuron of the SAM, also by the latter.
Understood in this way, deafferentation pain is effectively a pathogenetic type of neuropathic pain (Figure 2), with peculiar characteristics.
{kind=link}
Note that at the spinal level, due to the overlap of peripheral innervation territories, deafferentation pain only occurs if the lesion affects numerous neighboring dorsal roots and not if it affects only one, because in this case the afferents coming from the segments above and below the damaged dorsal root reach that metameric level via the Lissauer tract and the second neuron is not deafferented. On the contrary, with the involvement of Aβ fibers, pain always occurs in trigeminal deafferentation, since each portion of the retrogasserian root innervates only one facial area without overlap.
Another characteristic of deafferentation pain is the absence of allodynia 26 because, if it were present, it would have to be Aβ-mediated, since there is no reason for it to be C-mediated. However, if there is Aβ fiber activity, there may be deafferentation but no deafferentation pain, and if there is pain, it means that there is no Aβ fiber activity.
Conclusions
The term “deafferentation,” which does not appear in Bonica's historic 1953 treatise 27 and is not included in the IASP taxonomy,28 came into use in the late 1970s as a synonym for “denervation,” in reference to the consequences of nerve damage. It is noteworthy that a term coined solely to indicate a generic reduction or absence of afferents, and which, due to its appealing and high-sounding appearance, has been widely misused, both as a synonym for pain from generic nerve damage and, unfortunately, to indicate clinically uncertain situations that had nothing to do with it, “coincidentally” actually corresponds to a specific pathogenetic type of neuropathic pain. Recognizing the identity of deafferentation pain is important not only from the point of view of pathogenetic diagnosis but also in terms of therapeutic decision-making because, even though its treatment is the same as that used for axonal neuropathy pain, it is different from that of central pain. In the first case, drugs that act on the activation of the second neuron are appropriate, namely amitriptyline, duloxetine, and baclofen, and not gabapentinoids which, although acting on the second neuron, target the α2-δ receptor site of NMDA receptors that are not involved. In the second case, the only therapeutic option related to the pathogenetic mechanism is the restoration of GABAergic inhibition of the reticulothalamic nucleus on the dorsomedial nucleus to counteract its activation by the paleospinothalamic tract.
Conflict of interests
The author asserts that the article has been written in the absence of any conflict of interests.
Open Access-license (CC BY-NC 4.0)
Read Non-Commercial license
Published
30th October 2025
Bibliografia
1 Davar G, Maciewicz RJ. Deafferentation pain syndromes. Neurol Clin 1989 7:289-304.
2 Saitoh Y, Yoshimine T. Stimulation of primary motor cortex for intractable deafferentation pain. Acta Neurochir 2007; Suppl 97 (Pt 2): 51-56.
3 Ruiz-Juretschke F et al. Treatment of neuropathic deafferentation pain using DREZ lesions; long-term results. Neurologia 2011; 26: 26-31.
4 Hanakawa T. Neural mechanisms underlying deafferentation pain: a hypothesis from a neuroimaging perspective. J Orthop Sci 2012; 17: 331-335.
5 Hussein AE et al. Motor Cortex Stimulation for Deafferentation Pain. Curr Pain Headache Rep 2018; 22: 45.
6 Ahmed U, Baloch M. Deafferentation in Pain Medicine: A Narrative Review of Mechanisms and Management. J Pain Palliat Care Pharmacother 2025; 114-123.
7 Helme RD, Gibson S, Khalil Z. Neural pathways in chronic pain. Med J Aust 1990;153: 400-406.
8 Knecht S et al. Phantom sensations following acute pain. Pain 1998; 77: 209-213.
9 Marbach JJ, Raphael KG. Phantom tooth pain: a new look at an old dilemma. Pain Med 2000; 1: 68-77.
10 Rygh LJ et al. Cellular memory in spinal nociceptive circuitry. Scand J Psychol 2002; 43: 153-159.
11 Yamamoto T et al. Thalamic sensory relay nucleus stimulation for the treatment of peripheral deafferentation pain. Stereotact Funct Neurosurg 2006; 84: 180-183.
12 Di Rollo A, Pallanti S. Phantom limb pain: low frequency repetitive transcranial magnetic stimulation in unaffected hemisphere. Case Rep Med 2011: 130751.
13 Orlandini G. Patrimonio culturale dell’algologia e medicina del dolore. A. Delfino Ed, Roma 2025.
14 Sánchez-Ledesma MJ et al. Spinal cord stimulation in deafferentation pain. Stereotact Funct Neurosurg 1989; 53: 40-45.
15 Glynn CJ et al. Role of spinal noradrenergic system in transmission of pain in patients with spinal cord injury. Lancet 1986; 8518: 1249-1250.
16 Glynn CJ, Jamous MA, Teddy PJ. Cerebrospinal fluid kinetics of epidural clonidine in man. Pain, 1992; 49: 361-367.
17 Fenollosa P et al. Chronic pain in the spinal cord injured: statistical approach and pharmacological treatment. Paraplegia 1993; 31: 722-729.
18 Graff-Radford SB, Solberg WK. Atypical odontalgia. J Craniomandib Disord 1992; 6: 260-265.
19 Korczeniewska OA et al. Molecular mechanisms of painful traumatic trigeminal neuropathy-Evidence from animal research and clinical correlates. J Oral Pathol Med 2020; 49: 580-589.
20 Kerr FW. Central nervous system changes and deafferentation pain: the role of reorganization and gliosis. In Bonica JJ et al. Advances in pain research and therapy. Vol 5. Raven Press, New York 1983: pp.663-675
21 Rohof OJJM. Radiofrequency treatment of peripheral nerves. Pain Pract 2002; 3: 257-260.
22 Boivie J. Central Pain. In Wall PD and Melzack R. Textbook of pain. Third edition. Churchill Livingstone Interactive Publication, 1996.
23 Orlandini G. La semeiotica del dolore: dai presupposti teorici alla pratica clinica. Manuale d’uso pluridisciplinare. Prima edizione. Delfino Ed, Roma 2005.
24 Rinaldi PC, Young RF, Albe-Fessard D, Chodakiewitz J. Spontaneous neuronal hyperactivity in the medial and intralaminar thalamic nuclei of patients with deafferentation pain. J Neurosurg 1991; 74 : 415-421.
25 Albe-Fessard D. and Lombard M.C. Use of an animal model to evaluate the origin of and protection against deafferentation pain. In Bonica J.J.et Al. (Eds.). Advances in pain research and therapy. Vol.5. Raven Press, New York 1983: 691-700.
26 Sweet WH. Deafferentation pain after posterior rhizotomy, trauma to a limb, and herpes zoster. Neurosurgery 1984; 15: 928-932.
27 Bonica JJ. Management of pain. Lea and Febiger, Philadelphia, 1953.
28 IASP (Subcommittee on Taxonomy) Classification of chronic pain: description of chronic pain syndromes and definitions of pain terms. IASP Press, Seattle 1994.