Revisiting SCS: stimulation or conduction block?
Short review
Pathos 2025; 32.2. Online 2025, Sept 19
_________________________________________________________________________________
Guido Orlandini
Pain Medicine, Villa Ravenna (Chiavari, Ge)
_________________________________________________________________________________
Summary
As the name suggests, the concept of “stimulation” has always been fundamental to SCS, but a series of recent arguments are calling its validity into question. The mechanism of action of SCS has traditionally been interpreted as stimulation of the myelinated Aβ afferent fibres of the posterior columns, resulting in activation of the descending inhibitory pathway in the dorsolateral funiculus and the production of a multisegmental analgesic effect. Furthermore, stimulation of Aβ fibres penetrating the dorsal horn of the spinal cord is observed, followed by activation of inhibitory interneurons in the gelatinous substance and an effect on C fibres, inhibitory GABA-B receptors in the second neuron and the sympathetic origin neuron. HFSCS and Burst-SCS, which do not cause paraesthesia, appear to act through a distinct mechanism. This is not based on the stimulation of Aβ fibres but rather on the “inhibition” of the ascending multisynaptic system (AMS), with a multisegmental effect on neuropathic pain from axonal neuropathy, of the Lissauer tract. This has an effect on nociceptive pain and the sympathetic origin neuron, with a sympatholytic effect.
Riassunto
Come suggerisce il nome, per la SCS è sempre stato fondamentale il concetto di "stimolazione", ma una serie di recenti argomentazioni ne stanno mettendo in discussione la validità. Il meccanismo di azione della SCS è stato tradizionalmente interpretato come una stimolazione delle fibre afferenti mieliniche Aβ dei cordoni posteriori, con conseguente attivazione della via discendente inibitoria nel funicolo dorsolaterale e la produzione di un effetto antalgico plurisegmentale. Inoltre, si osserva una stimolazione delle fibre Aβ che penetrano nel corno dorsale del midollo spinale, seguita da attivazione degli interneuroni inibitori della sostanza gelatinosa e un effetto sulle fibre C, sui recettori GABA-B inibitori del secondo neurone e del neurone di origine del simpatico. La HFSCS e la Burst-SCS, che non provocano parestesie, sembrano agire attraverso un meccanismo distinto, non basato sulla stimolazione delle fibre Aβ ma piuttosto sulla "inibizione" del sistema ascendente multisinaptico (SAM), con un effetto plurisegmentale sul dolore neuropatico da neuropatia assonale, del tratto di Lissauer, con un effetto sul dolore nocicettivo e del neurone di origine del simpatico, con un effetto simpaticolitico.
Key words
SCS tradizionale, SCS ad alta frequenza, Burst-SCS
Parole chiave
Traditional SCS, High frequence SCS, Burst SCS
Introduction
The utilisation of rudimentary electrostimulation for the purpose of alleviating discomfort has a long and storied history, with origins that can be traced back to antiquity. The concept is referenced in third-millennium BCE Egyptian graffiti depicting a fish emitting electricity. In 46 AD, Scribonius Largus documented in his Compositione medicamentorum liber the efficacy of a live black torpedo ray in the treatment of headaches, recommending that patients apply the ray directly to the affected area. For individuals afflicted with gout, he advised that they stand on a torpedo ray until the lower leg becomes numb. Although electrostimulation has been utilised in a rudimentary form since antiquity, it only ceased to be an empirical treatment and became a codified clinical application when modern technology developed instruments capable of administering electricity in a controlled and measurable manner. This development has been termed the 'era of neuroadditive surgery'.
It is important to note that this terminology clearly emphasises a specific mechanism of action for these procedures: the addition of stimuli (stimulation and indirect inhibition), rather than the mechanism of direct inhibition. As Long observed, 1 the development of peripheral nerve stimulation (PNS) and spinal cord stimulation (SCS) in the latter half of the 1960s was not an arbitrary occurrence, but rather coincided with the dissemination of Melzack and Wall's, 2 seminal work on the gate control theory. Despite the fact that the gate control theory has never been definitively proven, and Wall himself stated in 1973 that 'the most conclusive and perhaps best thing that can be said about the 1965 publication is that it promoted debate and experimentation', its impact on medical culture was considerable.3
In 1967, Shelden 4 implanted the first electrode to stimulate the trigeminal nerve, and Shealy et al.5 implanted the first SCS electrodes. In 1973, Mazars et al.6 and Hosobuchi et al.7 independently proposed the concept of deep brain stimulation (DBS). In the subsequent year, Shealy 8 proposed the utilisation of transcutaneous electrical nerve stimulation (TENS) to evaluate the feasibility of implantation.9
Traditional SCS
SCS involves the implantation of electrodes in the epidural space. The first documented instance of this procedure was in 1967, when Shealy and colleagues 5 performed a thoracic laminectomy and implanted platinum plates that were sutured to the dura mater. This procedure became so widely used in the US during the second half of the 1960s that its indiscriminate use led to unsatisfactory results and a decline in interest in the method until the early 1970s. During this period, the percutaneous insertion of temporary electrodes was proposed as a means of testing patients prior to definitive implantation.10,11 Consequently, the percutaneous technique, which had been employed solely for testing, was subsequently adopted for definitive implantation.12 The initial proposal of spinal cord stimulation (SCS) was exclusively for the purpose of analgesia. However, it was subsequently recognised that SCS has the capacity to interfere with various autonomic functions. Its utilisation in the management of urinary retention in paraplegics13 has been documented, as has its application in the treatment of bladder incontinence,14 angina pectoris, and Raynaud's phenomenon in scleroderma. The utilisation of the aforementioned treatment has also been documented in the prevention of cerebral vasospasm-related damage.
It is evident that SCS exerts an analgesic effect in specific types of neuropathic pain, yet this effect is not observed in nociceptive pain. It has also been demonstrated to possess an autonomic-vasodilatory effect, which has significant applications in the treatment of peripheral artery disease and angina pectoris. Furthermore, due to its sympatholytic effect, SCS is an important contrast to CRPS in terms of pathogenesis.1
The hypotheses formulated to explain the mechanisms of action of SCS are summarised below: the theory of activation of large myelinated afferents; the theory of conduction block; and the theory of glial activation block.
The theory of the activation of large myelinated afferents
Despite the ongoing discourse surrounding the gate control theory in this context as if it were a religious tradition, it is implicated only in the mechanism of action of SCS with regard to Aβ fibres that run parallel to the dorsal horn of the spinal cord and activate the inhibitory interneuron of the gelatinous substance. In reality, this has a modest analgesic effect that only affects nociceptive pain conducted by C fibres. In the case of SCS, this is of negligible relevance as it does not affect the control of neuropathic pain from axonal neuropathy, which is of greater importance.
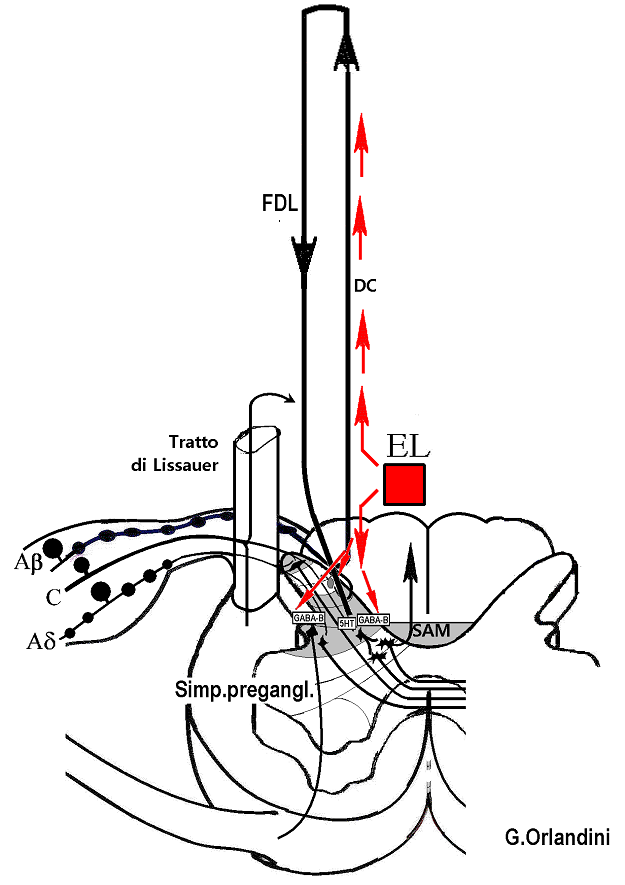
Notwithstanding the various gate control theories, the theory of the activation of large myelinated afferents remains the most widely accepted of the proposed theories. According to this theory, the activation of Aβ fibres located in the posterior columns of the spinal cord instigates the generation of orthodromic impulses. Upon reaching the nuclei of the gracile and cuneate fascicles, these impulses activate supraspinal centres, from which descending inhibitory pathways originate in the dorsolateral funiculus (DLF). Antidromic impulses are known to travel along collaterals directed to the superficial layers of the dorsal horn of the spinal cord (Figure 1). In both pathways, Aβ fibres have been observed to activate inhibitory interneurons in the dorsal horn of the spinal cord. The descending pathways in the dorsal lateral funiculus (DLF) have been shown to activate the 5-HT inhibitory receptors of the second neuron, thereby explaining the analgesic effect observed in cases of axonal neuropathic pain. The collaterals directed to the superficial layers of the dorsal horn of the spinal cord activate the inhibitory interneurons of the gelatinous substance, as well as the GABA_B receptors in the second neuron and the GABA_B receptors in the neuron of sympathetic origin. This phenomenon contributes to the analgesic effect observed in cases of axonal neuropathic pain.
{kind=link}
Theory of conduction block in Aδ and C fibers
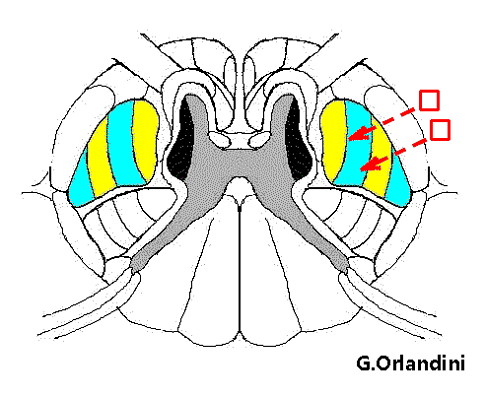
At a time when the analgesic effect of spinal cord stimulation (SCS) was widely accepted to be the result of the activation of large myelinated afferents, Larson et al.15 challenged this theory. The authors of the study reported the analgesic efficacy of electrostimulation of the anterior half of the spinal cord (Figure 2) and hypothesised that pain relief from SCS was due to conduction block in the spinothalamic tract rather than activation of the posterior columns. In accordance with this theoretical framework, Hoppenstein 16 successfully induced analgesia by utilising an electrical current of intensity 30 times lower when the electrodes were positioned in front of the lateral spinothalamic tract as opposed to their posterior placement. Furthermore, it was observed that, in the former case, the location of pain relief was contralateral to the site of stimulation.
{kind=link}
In accordance with the observations of Larson and Hoppenstein, it has been noted that patients undergoing percutaneous cervical cordotomy frequently report the temporary disappearance of contralateral pain as soon as the electrode penetrates the lateral spinothalamic tract during sensory stimulation at 75 Hz, even before the lesion is reached. During the same period, Campbell and Taub 17 and Ignelzi and Nyquist 18 formalised the hypothesis that electrostimulation reduces the number of impulses rather than adding impulses to the nerve, thereby causing a conduction block.
The conduction block hypothesis is supported by the observation of Campbell (1980) that increasing the intensity of electrical stimulation of a peripheral nerve initially raises the excitation threshold for tactile stimuli, followed by nociceptive stimuli, until the skin is completely anaesthetised. In light of the observations made, Campbell concluded that the hypothesis of neurostimulation activating large-calibre fibres was unfounded. Instead, he postulated that the phenomenon was more likely to be a result of conduction block in all afferent nerve fibres. Additionally, due to their greater surface-to-volume ratio, small-calibre fibres would be blocked at a lower stimulation frequency than that required for larger-calibre fibres.
Campbell 19 defined this phenomenon as a conduction block related to the stimulation frequency. In accordance with Adelman and Fitzhugh's 20 findings, the observed phenomenon was attributed to the accumulation of K⁺ ions surrounding the axon, leading to a reduction in the conductance of the Na⁺ channels. In practice, the stimulating current would collide with the electrical stimulus travelling orthodromically along the nerve fibres, thereby blocking it (the collision current theory). Furthermore, Campbell's observations on the utilisation of electrodes in the treatment of lumbosacral pain revealed a preference for placement behind the cauda equina as opposed to the spinal cord. From this position, it is improbable that the electrodes will activate the posterior cords; however, it is probable that they will block the conduction of the nociceptive fibres of the first neuron before they enter the spinal cord. Indeed, the conduction block theory can explain the analgesic effects of electrostimulating peripheral nerves or the anterolateral quadrant of the spinal cord or cauda equina, but not the posterior cords.
Theory of glial activation blockade
Finally, a few years ago, the involvement of glia was also hypothesized among the mechanisms of action of SCS. Used at frequencies between 4-60 Hz, SCS would block glial activation in the spinal cord 21 and thus the pathological activation of the second neuron by Aβ fibers responsible for pain from somatic neuropathy.22 In this case too (unless we hypothesize the action of some inhibitory interneuron), it would not be stimulation but inhibition.
High-frequency SCS and Burst-SCS: the “crisis” caused by new technological acquisitions
In comparison to the approach that was almost unquestioningly accepted until around 15 years ago, SCS must now be re-examined in light of new technological advances, such as high-frequency SCS and Burst SCS. The efficacy of these techniques in treating lumbar pain, which is often not clearly defined but is likely to be of a nociceptive nature, is well-documented. Furthermore, these techniques are easier to implement as they do not require the patient to cooperate by searching for paresthesia. Consequently, these procedures can be performed under the administration of general anaesthesia.
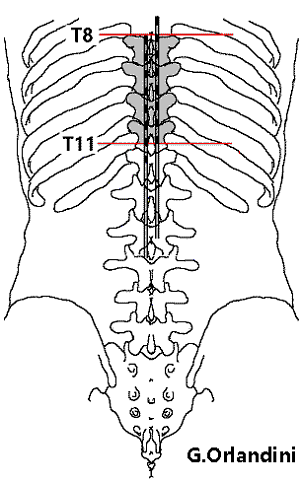
Figure 3 – Electrode placement in high-frequency SCS
In order to facilitate the management of lumbosacral and lower limb discomfort, it is imperative to employ a double octopolar electrode configuration, meticulously positioned between the eighth and eleventh thoracic vertebrae. The initial contact of one electrode is to be situated at the uppermost border of the eighth thoracic vertebra's body, while the final contact of the second electrode is to be placed at the lowermost border of the eleventh thoracic vertebra's body (Figure 3). In order to facilitate the management of cervicobrachial and upper limb discomfort, it is recommended that a double octopolar electrode be positioned between C2 and C7 at the midline. This approach has been shown to minimise the potential for electrode displacement, thereby reducing the occurrence of undesirable variations in paresthesia intensity associated with alterations in position.
{kind=link}
The issue that remains to be resolved is the understanding of whether these novel techniques exert a "stimulation" and an "indirect inhibition" or whether they do something completely different. It is disconcerting that instead of developing new technologies to achieve a goal, we are compelled to question the mechanisms by which they achieve that goal.
Firstly, the question of whether high-frequency SCS and Burst SCS are synonymous remains unresolved. However, DeRidder et al. 23 posit that both modalities act by modulating the medial pain pathways, a term that remains undefined and may signify a reduction in nociceptive afferent fibre activity or an increase in the activity of fibres that activate inhibitory circuits. The two techniques would thus be equivalent insofar as they do not cause paresthesia, due to the low intensity of the current supplied being insufficient to activate the Aβ afferents of the posterior cords.
The majority of observers concur that high-frequency SCS is more efficacious than conventional SCS. Moreover, frequent reports indicate that, in contrast to traditional SCS, high-frequency SCS effectively controls lumbar pain.24-30
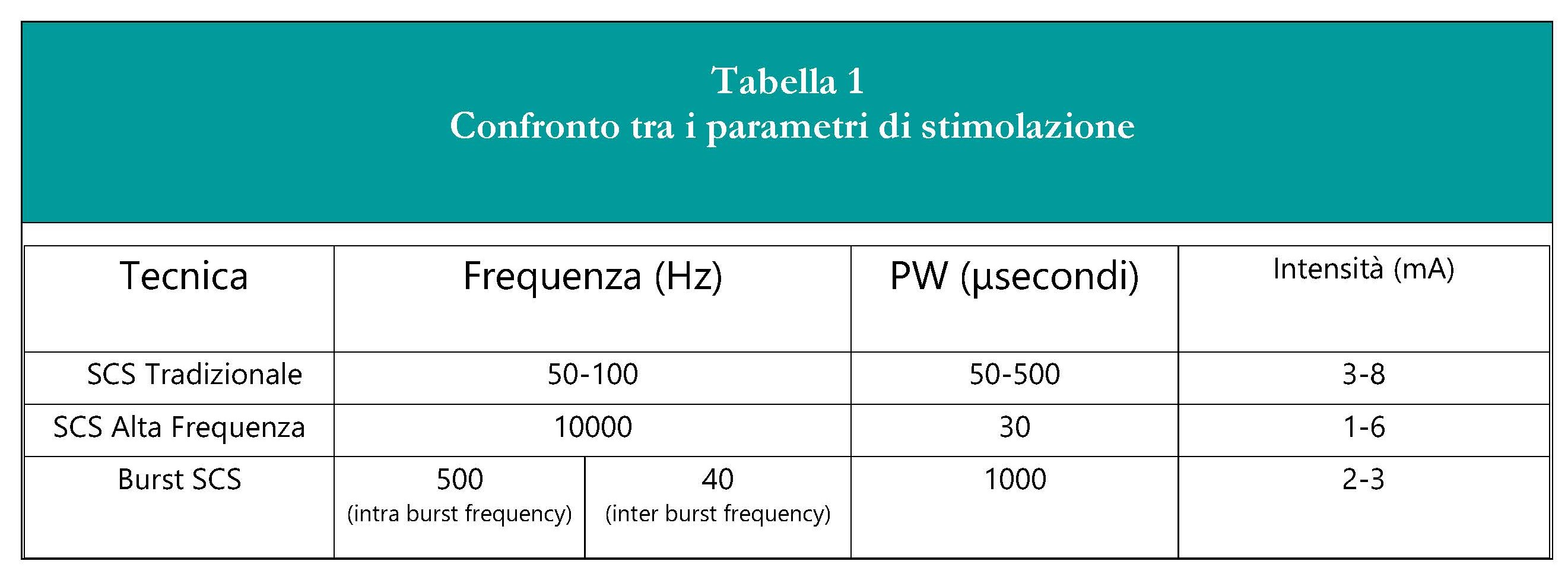
Burst SCS, first reported by DeRidder 31 consists of packets of 5 pulses with a frequency of 500 Hz and a PW of 1000 μsec that are sent 40 times per second, i.e. at intervals that mimic the natural tendency of the CNS to discharge and would produce an analgesic effect by "synchronizing" with them (Table 1).32,33
{kind=link}
Frequency (Hz) PW (μseconds) Intensity (mA)
Traditional SCS 50–100 50–500 3–8
High-frequency SCS 10,000 30 1–6
Burst SCS 500
(intra-burst frequency) 40
(inter-burst frequency) 1,000 2–3
Tabella 1 – Confronto fra i parametri della stimolazione nella SCS tradizionale, nella SCS ad alta frequenza e nella Burst SCS. Notare che l’intensità di corrente nella SCS ad alta frequenza è la metà di quella della SCS tradizionale
A thorough review of the extant literature on the subject reveals a paucity of clarity regarding the operational mechanisms of these novel techniques. The prevailing sentiment that emerges from this examination is one of disinterest in this particular aspect, suggesting a lack of engagement and exploration of the underlying principles. A review of the literature on the mechanisms of action reveals that Burst SCS exerts its effect by reducing the discharge of WDR-n in the CDMS. 34. Furthermore, it has been established that both high-frequency SCS and Burst SCS function by modulating the medial pain pathways [Bocci et al., 2018; Ahmed et al., 2018]. Additionally, it has been determined that the intensity of the current delivered to implement high-frequency SCS is lower than that required to activate large myelinated afferents and thus evoke paresthesias. However, it is sufficient to induce conduction block in small C fibres at the segmental level (perhaps in the Lissauer tract), which would be responsible for the analgesic effect.
Reassessment of the conduction block theory
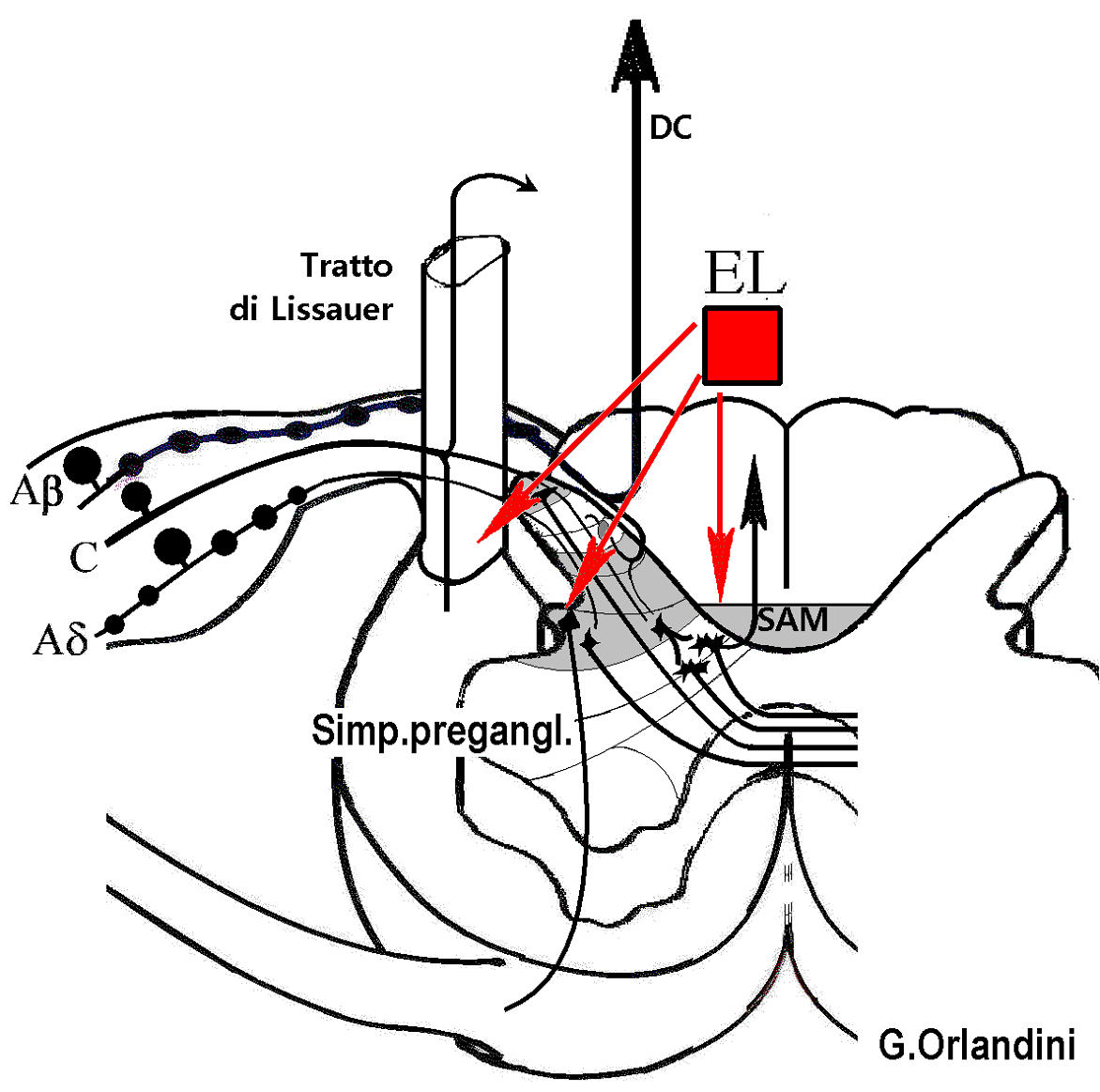
In the case of high-frequency SCS and Burst-SCS, it appears imperative to postulate a distinct mechanism of action, divergent from that of Aβ fiber activation. Consequently, attention must be directed towards the mechanism of conduction block, not of Aβ fibers but of C fibers in the central pathways (Figure 4), i.e., in the ascending multisynaptic system (AMS). In summary, it can be hypothesised that, in the absence of activation of the Aβ fibres that ascend in the posterior columns and therefore of activation of the inhibitory mechanism that descends in the DLF, the analgesic effect of high-frequency SCS is due, as regards axonal neuropathy pain, to conduction block in the AMS, as regards nociceptive pain, to conduction block in Lissauer's tract (with segmental effect) and as regards sympathetic block, to block of the activation of neurons of sympathetic fiber origin (with segmental effect).
{kind=link}
Conclusioni
In view of the aforementioned considerations, it would appear that the term "stimulation" should be subjected to closer scrutiny. It is intuitively obvious when applying electrical current to a peripheral nerve, yet simultaneously misleading because it is quite different if, with the application of exogenous electrical current, the electrical activity in the nerve is increased (i.e., its "conduction is increased" and therefore "stimulating" it) or reduced (i.e., "blocking conduction"). Conversely, the substitution of the term "nerve stimulation" with "nerve conduction block" suggests the acknowledgement of a well-defined mechanism of action. Moreover, given the functional interruption of afferents for SCS, this approach conceptualises SCS as being more akin to neurolesive techniques, with the capacity to selectively act on the SAM. Consequently, this would render SCS effective in the management of pain from axonal neuropathy and potentially from deafferentation on the Lissauer tract. This would also make it effective in the management of nociceptive lumbar pain, as well as exerting a direct sympatholytic effect on cells of sympathetic origin.
Conflitto di interessi
The author asserts that the article has been written in the absence of any conflict of interest.
Open Access-license (CC BY-NC 4.0)
Read Non-Commercial license
Published
19th September 2025
Bibliografia
1. Adelman WF, Fitzhugh R. Solution of the Hodgkin-Huxley equations modified for potassium accumulation in a periaxonal space. Fed Proc 34 (1975) 1322-1329.
2. Ahmadi SA, Vesper J, Schu S, Slotty P.J. High-Frequency Spinal Cord Stimulation in Surgery-Naïve Patients-A Prospective Single-Center Study. Neuromodulation, 20 (2017) 348-353.
3. Ahmed S, Yearwood T, De Ridder D, Vanneste S. Burst and high frequency stimulation: underlying mechanism of action. Expert Rev Med Devices 2018; 15: 61-70.
4. Al-Kaisy A, Palmisani S, Smith TE, Carganillo R et al. Long-Term Improvements in Chronic Axial Low Back Pain Patients Without Previous Spinal Surgery: A Cohort Analysis of 10-kHz High-Frequency Spinal Cord Stimulation over 36 Months. Pain Med 2018;19: 1219-1226.
5. Al-Kaisy A, Palmisani S, Smith TE, Pang D et al. 10 kHz High-Frequency Spinal Cord Stimulation for Chronic Axial Low Back Pain in Patients With No History of Spinal Surgery: A Preliminary, Prospective, Open Label and Proof-of-Concept Study. Neuromodulation 2017;20: 63-70.
6. Al-Kaisy A, Van Buyten JP, Smet I, Palmisani S et al. Sustained effectiveness of 10 kHz high-frequency spinal cord stimulation for patients with chronic, low back pain: 24-month results of a prospective multicenter study. Pain Med 2014;15: 347-354.
7. Augustinsson LE, Carlsson CA, Fall M. Autonomic effects of electrostimulation. Appl Neurophysiol 1982; 45: 185-189.
8. Bocci T, De Carolis G, Paroli M, Barloscio D et al. Neurophysiological Comparison Among Tonic, High Frequency, and Burst Spinal Cord Stimulation: Novel Insights Into Spinal and Brain Mechanisms of Action. Neuromodulation 2018 21(5):480-488.
9. Burton CV. Transcutaneous electrical nerve stimulation to relieve pain. Postgrad Med 1976; 59: 105-108.
10. Cedeño DL et al. Modulation of Glia-Mediated Processes by Spinal Cord Stimulation in Animal Models of Neuropathic Pain. Front Pain Res (Lausanne) 2021; 2: 702906.
12. Cook AW, Oygar A, Baggenstos P, Pacheco S. et al. Vascular disease of extremities. Electric stimulation of spinal cord and posterior roots. NY Sate J Med 1976; 76: 366-368.
13. Deer T, Pope J, Hayek S, Narouze S et al. Neurostimulation for the treatment of axial back pain: a review of mechanisms, techniques, outcomes, and future advances. Neuromodulation 2014; 17 Suppl 2: 52-68.
14. DeRidder D et al. Burst spinal cord stimulation: toward paresthesia-free pain suppression. Neurosurgery 2010; 66: 986-90.
15. Hoppenstein R. Percutaneous implantation of chronic spinal cord electrodes for contro of intractable pain: preliminary report. Surg Neurol 1975b; 4:195-198.
16. Hosobuchi Y, Adams JE and Weinstein P.R. Preliminary percutaneous dorsal column stimulation prior to permanent implantation. J Neurosurg 1972; 37: 242-245.
17. Kilchukov M et al High-Frequency versus Low-Frequency Spinal Cord Stimulation in Treatment of Chronic Limb-Threatening Ischemia: Short-Term Results of a Randomized Trial. Stereotact Funct Neurosurg 2023; 101: 1-11.
18. Kinfe TM et al. High Frequency (10 kHz) or Burst Spinal Cord Stimulation in Failed Back Surgery Syndrome Patients With Predominant Back Pain: Preliminary Data From a Prospective Observational Study. Neuromodulation 2016; 19: 268-75.
19. Larson SJ, Sances A, Cusick J, Meyer GA and Swiontek TA. Comparison between anterior and posterior spinal implant systems. Surg Neurol 1975; 4: 180-186.
20. Larson SJ, Sances A, Riegel DH, Meyer GA et al. Neurophysilogical effects of dorsal column stimulation in man and monkey. J Neurosurg 1974; 41: 217-223.
21. Long DM. Electrical stimulation for the control of pain. Arch Surg 1977;112: 884-888.
22. Melzack R and Wall PD. Pain mechanisms: a new theory. Science, 1965; 150: 971-978.
23. Murphy DF and Giles KE. Intractable angina pectoris: management with dorsal column stimulation (case report). Med J Aust 1987; 146: 260.
24. Pain Pract 2023 Mar;23 (3):301-312.doi: 10.1111/papr.13184. Epub 2022 Dec 8.
25. Rapcan R., Mlaka J., Venglarcik M., Vinklerova V., Gajdos M., Illes R. High-frequency - Spinal Cord Stimulation. Bratisl Lek Listy., 116 (2015) 354-356
26. Ray C.D. Electrical stimulation: new method for therapy and rehabilitation. Scand. J. Rehab. Med., 10 (1978) 65-74
27. Russo M. and VanBuyten J.P. 10-KHz High-frequency SCS therapy: a clinical summary. Pain Medicine, 16 (2014) 934-942
28. Sato K.L. et al. Spinal cord stimulation reduces mechanical hyperalgesia and glial cell activation in animals with neuropathic pain. Anesthesia and Analgesia, 118 (2014) 464-472
29. Shealy C.N., Mortimer J.T. and Reswick J. Electrical inibition of pain by stimulation of the dorsal column: preliminary clinical reports. Anesth.Analg., 46 (1967) 489
30. Shelden C.H., Pudenz R.H. and Doyle J. Electrical control of facial pain. Am. J. Surg., 114 (1967) 209-212
31. Van Havenbergh T., Vancamp T., Van Looy P., Vanneste S., De Ridder D. Spinal cord stimulation for the treatment of chronic back pain patients: 500-Hz vs. 1000-Hz burst stimulation. Neuromodulation, 18 (2015) 9-12
32. VanBuyten J.P., Al-Kaisy A., Smet I., Palmisani S., Smith T. High-frequency spinal cord stimulation for the treatment of chronic back pain patients: results of a prospective multicenter European clinical study. Neuromodulation, 16 (2013) 59-65
33. Wall P.D. Dorsal horn electrophysiology. In Iggo A. (Ed.). Handbook of sensory physiology. Vol.2. Sormatosensory System. Springer-Verlag, Berlin 1973, pp.253-270
34. Zina G., Puiatti P., Vignotto F. and Maritano M. Epidural spinal cord electrical stimulation in progressive systemic sclerosis. In Burgdorf W.H.C. and Katz S.I.(Eds.). Dermatology: Progress & Perspectives. The Proceedings of the 18th World Congress of Dermatology, New York, June 12-18, 1992, pp.447-450.