WinAlgos: software for algologists
Medicine and Informatics
Pathos 2024; 31. 3. Online 2024, Nov 30
_________________________________________________________________________________
Guido Orlandini
Medicina del dolore, Villa Ravenna (Chiavari, Ge)
Synlab Institute (Monza)
Mauro Montagni
Informatic Engineer (Chiavari, Ge)
_________________________________________________________________________________
Summary
WinAlgos is a software that was first developed in 2001 as a "computerised algological record" and later evolved into 2022 version as a tool to assist the algologist in examining patients and formulating accurate pathogenetic and syndromic diagnosis of pain.
Riassunto
WinAlgos è un software nato nel 2001 come "cartella algologica computerizzata" ed evoluto successivamente, nella versione 2022, come procedura per supportare l’algologo nella visita del paziente e nella formulazione della diagnosi patogenetica e sindromica del dolore.
Key words
Algology, examination, pain pathogenesis, syndromic diagnosisParole chiave
Algologia, visita, patogenesi dolore, diagnosi sindromica
Introduction
The need to use information technology to collect patients' clinical data and to store them in convenient paperless archives, where they can be quickly re-examined during subsequent visits and compared for research purposes, led one of the authors (Guido Orlandini) to design an Algological Clinical File in 2001, which was then implemented and named WinAlgos by an IT expert (engineer Mauro Montagni) in a very detailed version which (also translated into English) was much appreciated and used not only in Italy, but at the same time was little used because it was considered too complex at a time when familiarity with computers was still rather limited.1
Twenty years later, WinAlgos (simplified) has been transformed from a simple clinical file into an application that not only guides the algological examination, but also serves as a tool for the guided formulation of the pathogenetic and syndromic diagnosis of pain.
Matherials and methods
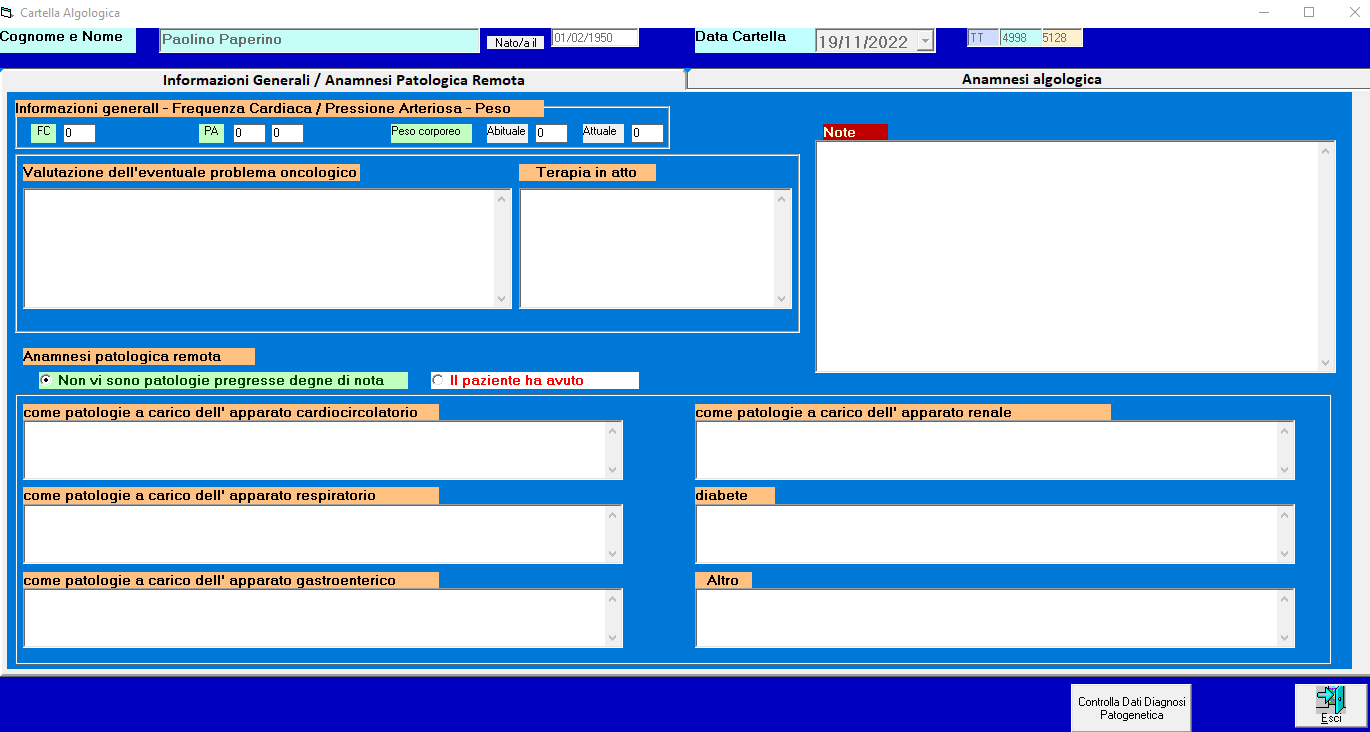
The programme (which can be viewed at www.winalgos.com) is developed in a series of steps that begin with the collection of the patient's biographical data, continue with guidance for a brief remote pathological history and verification of any, current, associated pathologies (Figure 1) and then with guidance for the algological examination.
{kind=link}
For illustrative purposes, the figures here detail the steps of the procedure with reference to the frequent situation of a Lumbosacral Radiculopathy.
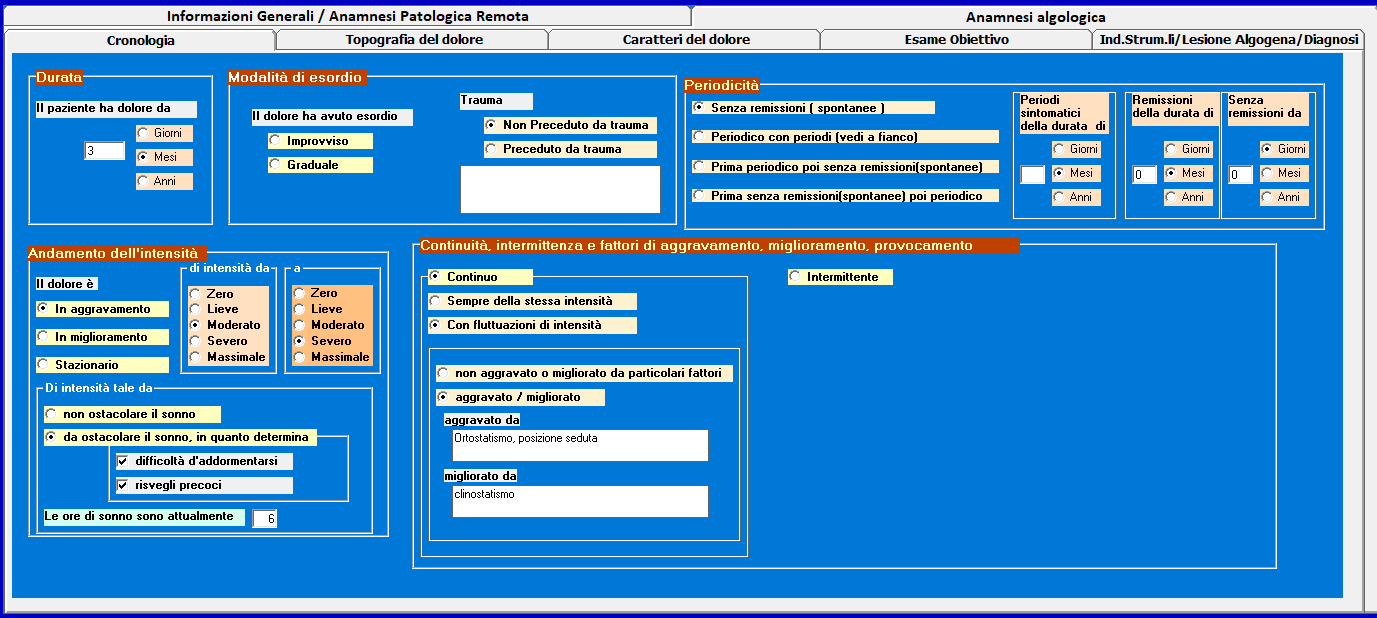
It begins with a guided algologically anamnesis, which includes the study of chronology, topography and characteristics of the pain.
The study of chronology of pain involves the evaluation of duration of the pain, mode of onset (sudden or gradual, preceded or not by trauma), periodicity (without remission or periodic), course of intensity (worsening, improving or stationary), its continuity or intermittence (Figure 2).
{kind=link}
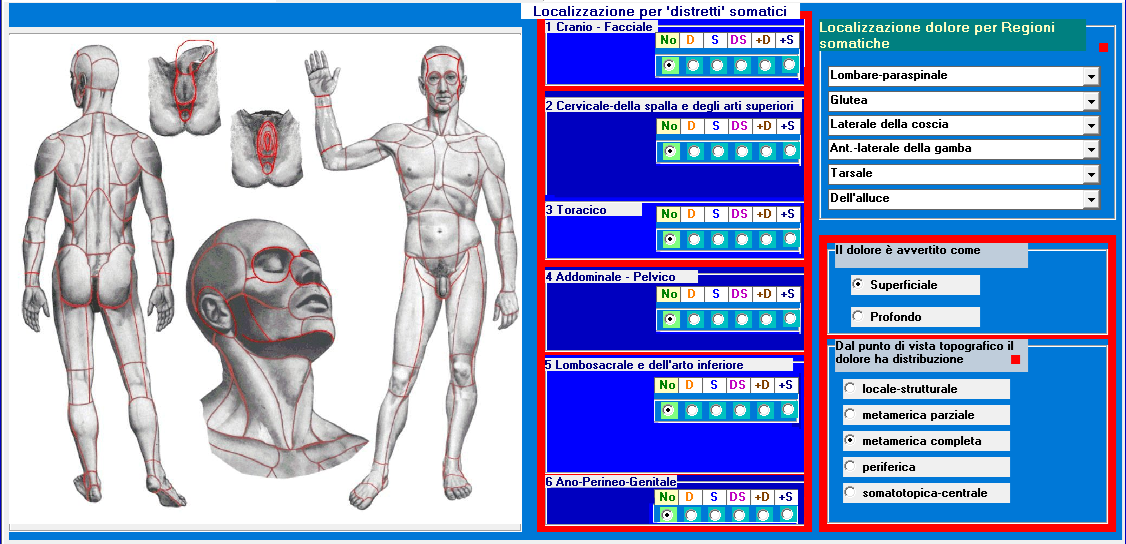
The study of the topography of pain involves choosing from a figure of human body the somatic region(s) involved, together with the affected side (Figure 3) and assessing the superficial or deep character and type of topographical distribution.
{kind=link}
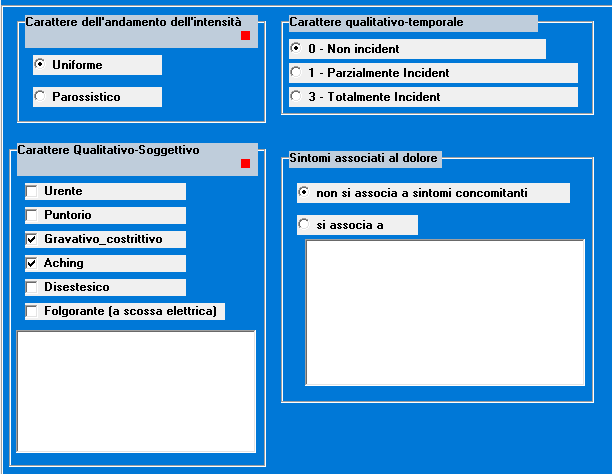
The study of pain characters involves the detection of character of intensity pattern (uniform or paroxysmal), the subjective qualitative character (aching, puncture, gravative, etc.), the qualitative-temporal character (non-incident or incident) and annotation of any complaints associated with the pain (Figure 4).
{kind=link}
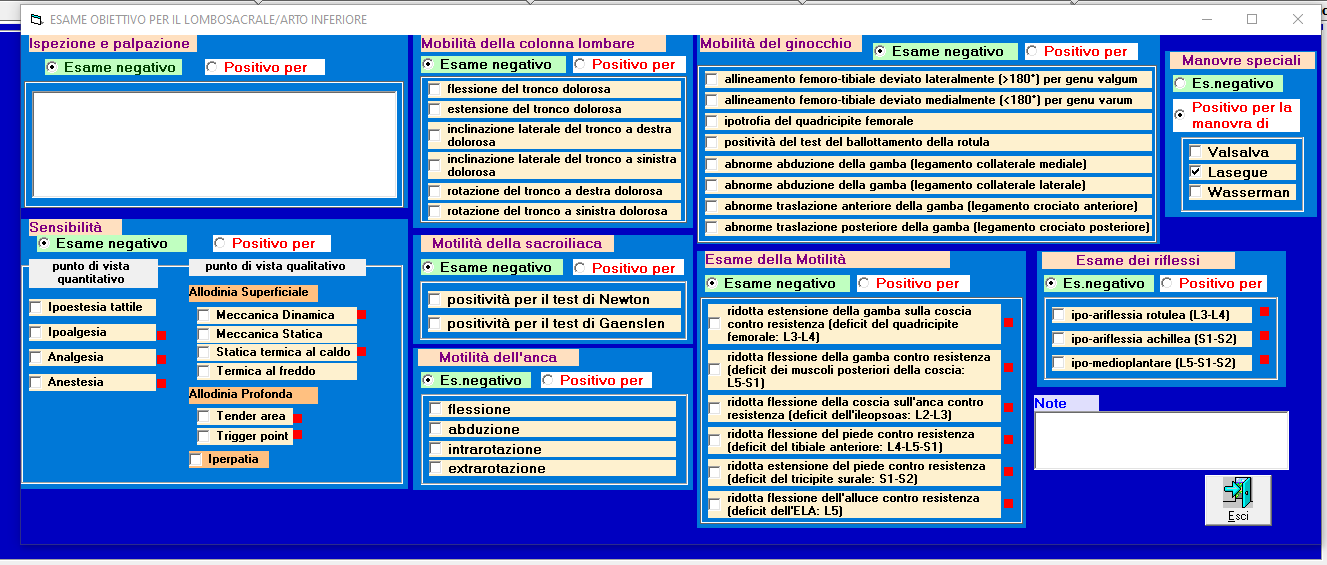
Once the anamnesis is concluded, one proceeds with the objective algological examination of the somatic district(s) identified with the algological anamnesis.
We begin by noting the findings obtained by inspection and palpation and proceed with the examination of sensitivity from a quantitative point of view, highlighting any deficits, and from a qualitative point of view highlighting superficial and deep allodynia (trigger points and tender areas), motility, osteotendin reflexes (specific according to the somatic district under examination) and special semeiological manoeuvres for the individual districts (Figure 5).
{kind=link}
Objective examination
At this point, the results of any instrumental investigations are noted down and finally computer will analyse the various findings to propose a pathogenetic diagnosis of pain (Figure 6) and suggest the possible syndromic diagnosis(s) (Figure 7): this is the most interesting and innovative part of WinAlgos which, as we have said, is not only a collection of data gathered in a medical record but also claims to elaborate and propose the algological diagnosis.
{kind=link}
{kind=link}
By recording the data obtained from the algological examination, we have provided the computer with a series of information, part of which constitutes the ‘Evaluation Criteria’ that are mutually correlated and almost always lead to a definite pathogenetic diagnosis or at least to a motivated diagnostic suspicion.
Algorithm for diagnosis
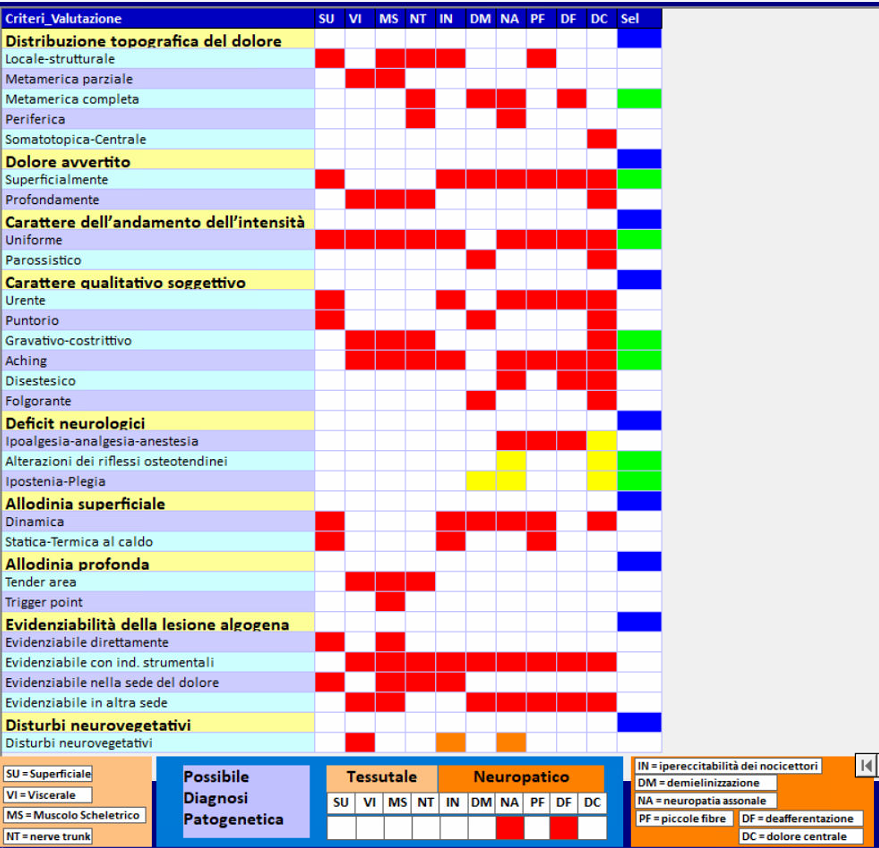
The algorithm used by the programme to formulate the pathogenetic diagnosis (Figure 6) is based on a scheme proposed in several publications.2-3-4 which involves considering a series of evaluation criteria that are: "topographical distribution of pain", "pain felt superficially or deeply", "character of the trend of pain intensity" (uniform or paroxysmal), "qualitative-subjective character of pain" (burning, puncture, gravitative-constrictive, etc.), "qualitative-subjective character of pain" (pain that is not felt in the body, but that is felt in the brain, etc.), “neurological deficits”, “superficial allodinia”, “deep allodinia”, “detectability of the algogenic lesion” and “neurovegetative disorders”.
Some of the reasoning that the Algologist (or the computer on his behalf) has to do to arrive at the pathogenetic diagnosis of pain is given here.
Considering the distribution of pain, local-structural type depicts superficial cutaneous-mucosal tissue pain, deep musculoskeletal tissue pain or nerve trunk pain or otherwise neuropathic pain from persistent nociceptor hyperexcitability or small-fibre pathology; partial metameric distribution depicts deep visceral or somatic tissue pain and excludes neuropathic pain; complete metameric distribution excludes all tissue pain and points towards neuropathic pain which cannot be that from persistent hyperexcitability of nociceptors or from small-fibre damage and must point towards demyelination, axonal neuropathy and especially deafferentation pain; peripheral distribution depicts neuropathic pain from injury in a peripheral nerve.5
Pathogenetic diagnosis of pain
Pain felt deeply is undoubtedly tissue pain and cannot be neuropathic (with the exception of central pain), whereas pain felt superficially, if it is not superficial tissue pain from a skin or mucosal lesion, is definitely neuropathic.
Considering the criterion of intensity pattern, paroxysmal character (typical of trigeminal neuralgia) excludes all types of tissue and neuropathic pain with the exception of demyelination pain.
Within the criterion of subjective qualitative character, only the gravative-constrictive character that depicts deep tissue pain, the dysesthetic character that depicts a generic neuropathic pain, and above all the dysesthetic character that is strongly suggestive of demyelinating pain are relevant.
The criterion of the detectability of the algogenic lesion is relevant whether the lesion is at the site of pain denouncing superficial cutaneous-mucosal or deep musculoskeletal tissue pain and in relation to whether it is detectable at the site of pain (denouncing a primary pain) or elsewhere (denouncing a secondary pain).
The criterion of the presence of neurological deficits is relevant in that it eliminates the possibility of pain being tissue-based and points towards neuropathic pain, excluding pain from persistent nociceptor hyperexcitability, pain from demyelination and pain from small-fibre damage, and making axonal neuropathy pain or deafferentation pain (if it affects the trigeminal territory) highly probable.
Last, but of great importance, is the criterion of allodynia detection. The detection of superficial allodynia must lead one to assess the possibility of superficial cutaneous or mucosal tissue pain: if this possibility is excluded, it points towards pain from persistent nociceptor hyperexcitability, demyelination or axonal neuropathy, while excluding pain from small-fibre damage and deafferentation.
The finding of deep allodynia is obtained with the palpation part of the objective examination. Tender areas and myofascial trigger points should be considered deep allodynia. This finding should lead one to consider the possibility of visceral tissue, musculoskeletal or nerve trunk pain if it corresponds to a tender area and musculoskeletal tissue pain if it corresponds to a trigger point. The presence of a tender area must be considered in the case of pain caused by palpation of the abdomen in search of a visceral lesion, as well as pain caused by movement in the case of a musculoskeletal lesion (e.g. in coxarthrosis and gonarthrosis, supraspinatus tendonitis, etc.).
Syndromic diagnosis
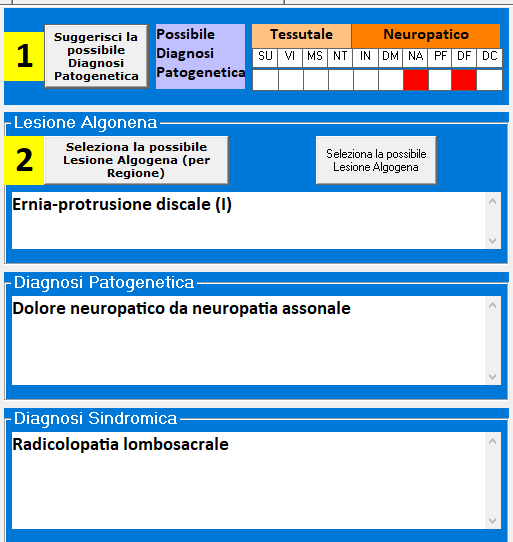
Once the pathogenetic diagnosis has been formulated, the algorithm will propose possible syndromic diagnoses (Figure 7) based on the site of the pain and the identification of the algogenic lesion, but it is the Algologist who selects the correct one.
With regard to syndromic diagnosis, it should be borne in mind that, although the primary objective of the algologist is to search for the pathogenesis of pain and in some circumstances this is sufficient to direct antalgic treatment, it may be important to identify the site of algogenic lesion in anticipation of a non-pharmacological but infiltrative or surgical treatment. For example, if one has recognised a deep musculoskeletal tissue pain felt in the upper limb in the deltoid region, instead of only proceeding with the appropriate treatment to counteract the pathogenic mechanism that sustains that pain, if one can identify the algogenic lesion in the supraspinatus tendon by completing the pathogenic diagnosis with the syndromic one, one can selectively act on that pathology. Considering other clinical situations, if in a patient with lumbar pain we reach the pathogenetic diagnosis of deep musculoskeletal tissue pain, we must complete the investigation to identify the site of the algogenic lesion because the treatment is different if it is at the level of an intervertebral disc, facet joint, ligament or muscular structures; in the case of an epigastric pain radiating to the upper lumbar region, which we identify as deep visceral tissue, the investigation must be completed with the search for the algogenic lesion that could be, for example, in pancreas and require not only antalgic treatment but also and above all direct treatment on the pancreatic lesion. Furthermore, it should be borne in mind that syndromic diagnosis is convenient for communication purposes.
Finally, the programme provides for a diary where subsequent algological visits are recorded for each patient with the therapeutic prescriptions and procedures performed, the assessment of pain intensity and the possibility of drawing up a clinical report.
Conclusions
Assuming that Algologist is not only the Pain Therapist and his task is not simply to perform pain therapy but first and foremost to make the pathogenetic and syndromic diagnosis and choose the treatment, the aspiring Algologist must have a set of knowledge derived, rather than from different specialisations, from medical knowledge in general that constitute what we can call the “cultural heritage of Algology”. Having reaffirmed the concept that “Algology” is the study of neuroanatomy, physiology and pathogenesis of pain and “Pain Medicine” (which the includes algological examination, the therapeutic decision and the execution of therapy) is the clinical application of Algology, the Algologist is the physician who knows Algology and is therefore able to practice Pain Medicine. It is on these premises that WinAlgos was conceived and realised, which started out as a simple Algological Clinical File and then evolved into a system that is intended to be a support for the formulation of the algological diagnosis.
At this point, one cannot help but draw attention to the much-fashionable Artificial Intelligence (AI), which has been very much in the news media in recent months, especially the “generative” one, i.e. the one capable of producing texts, images, videos and answers based on a question asked in the form of written text or voice recognition. What we are most interested in with reference to WinAlgos, however, is the part of artificial intelligence called ML (machine learning) and in particular the part called “deep learning” which deals with creating systems that learn or improve their performance based on the data used. Such techniques use artificial neural networks that attempt to replicate the behaviour of the human brain. This is actually an oversimplification since such systems are subject to technical constraints not present in biological systems. However, starting from large databases of specific data, supervised and validated by experts, the “artificial” neural network attempts to process real-time responses to user requests. In other words, this tool uses algorithms that, modelled on the decision-making processes of the human brain, can “learn” from the available data and make increasingly accurate predictions as the accuracy of the data increases. This is nothing new because for decades, computer science has been able to highlight connections and relationships in data at times that are difficult for humans to achieve. What has changed is the ability to process data in terms of hardware power (and thus processing speed) and above all the introduction of new algorithms based on the imitation of biological neural networks.
At this point, let us refer to what a doctor does every time he tries to make a diagnosis. Based on his experience, he assesses the symptoms, searches for possible inconsistencies in both the symptoms and the available instrumental inadequacies, and begins to work out the possible diagnosis. The more experience the doctor has, i.e. the more data he has memorised during his professional life (including any mistakes made in previous diagnoses), the more correctly he will be able to establish the diagnosis and treatment. Thinking now of being able to multiply the experience of the individual doctor by a large number of doctors willing to provide feedback on their experiences by storing them in a device such as WinAlgos, one realises how powerful and useful such technology could become.
For example, if one tries to use the free version of “Copilot”, one is initially surprised to get answers that are interesting at first glance, but then, going into detail, one finds that (even if they are very well summarised) they are absolutely generic and approximate, which the layman can get from internet searches... and that can only be so, since that is the data base for processing!
In fact, in order to get correct and really useful answers, the basis of the elaborations must be as reliable and validated as possible. At the moment, for the Algologist, the possibility of having such a tool to aid diagnosis seems a long way off, but in other areas of medicine (perhaps more codified and better funded) it is no longer just science fiction.
While waiting to organise a dedicated database, WinAlgos uses computer techniques that are more classical but not, if well managed, less interesting. While AI uses techniques that, simplifying, we could call statistical, WinAlgos for now uses procedural and deterministic techniques in the sense that the answers are uniquely determined by tables and algorithms used to generate the diagnosis. For example, for the formulation of the pathogenetic diagnosis, WinAlgos compares the evaluation criteria summarised in the table in Figure 6 with the findings in a series of tables, which should be further implemented as the programme is used by as many healthcare professionals as possible, thus becoming a system that is continually being improved.
Conflict of interest
Gli autori dichiarano assenza di conflitto di interessi
Open Access-license (CC BY-NC 4.0)
Read Non-Commercial license
Published
30th November 2024
Bibliografia
1) Montagni M. L’informatizzazione in terapia antalgica. In Orlandini G. (Ed). Atti dell’Incontro Residenziale di Aggiornamento sul “Linee guida in algologia: criteri organizzativi, semeiotica e metodologia diagnostica, indicazioni delle tecniche neurolesive e di neuromodulazione. Casale Monferrato (AL) 17-18 settembre 1999, Atti, pp101-116.
2) Orlandini G. La semeiotica del dolore: dai presupposti teorici alla pratica clinica. Manuale d’uso pluridisciplinare. Seconda Edizione. Delfino Ed, Roma 2014.
3) Orlandini G. La decisione terapeutica nella medicina del dolore: dalla diagnosi patogenetica alla scelta motivata della terapia. Delfino Ed, Roma 2020.
4) Orlandini G. Manuale della visita algologica e della formulazione della diagnosi. Delfino Ed, Roma 2022.
5) Melzack R and Torgerson WS. On the language of pain. Anesthesiology, 34 (1971) 50-59.
6) Blumberg ML, Ostrum BJ, Ostrum DM. Changes in MR signal intensity of the intervertebral disc. Radiology, 179 (1991) 584-585.
7) Cox JM. Spinal stenosis. In: Cox JM(Ed). Low back pain: mechanism, diagnosis, and treatment. Williams & Wilkins, Baltimore, Philadelphia, London, Paris, Bangkok, Buenos Aires, Hong Kong, Munich, Sydney, Tokyo, Wroclaw, 1999, pp.169-207.
8) Travell JG. and Simons DG. Myofascial pain and dysfunction: the trigger point manual. Vol 1. The upper extremities. Williams & Wilkins, Baltimore, London, Los Angeles, Sydney 1983.
9) Rae P, Venner RM, Waddel GA. Simple clinical technique of measuring lumbar flexion. Journal of the Royal College of Surgeons of Edinburgh, 29 (1984) 281-284.