Ozone therapy in a patient with epicondylitis and bone oedema
Clinical report
Pathos 2024; 31. 3. Online 2024, Nov 15
_________________________________________________________________________________
Antonino Genovese, Graziella Tindera Giuffrè,
Dario Iannelli, Filippo Iannelli,
Anaesthesia and Pain Therapy,
Centri Iannelli Diagnosi, Barcellona P.G. (ME), Italy
_________________________________________________________________________________
Summary
Epicondylitis is a debilitating condition of the elbow. The pain in the upper extremity is usually sharp and excruciating, limiting mobility and affecting work activity and quality of life. The patient usually reports unilateral attacks of pain that begin abruptly and last for varying lengths of time. The authors present a clinical case of a 48-year-old patient suffering from epicondylitis and bone oedema secondary to sports overuse. This study shows that treatment with Ozone therapy proved effective in both pain control and reduction of bone oedema.
Riassunto
L’epicondilite è un disturbo del gomito gravemente invalidante. Il dolore dell'arto superiore è solitamente acuto e lancinante e ne limita la motilità, con ripercussioni sull'attività lavorativa e la qualità della vita. Solitamente, il paziente riferisce attacchi di dolore unilaterali che iniziano bruscamente e durano per periodi di tempo variabili. Gli autori presentano un caso clinico che coinvolge un paziente di 48 anni affetto da epicondilite ed edema osseo secondario a sovraccarico sportivo. Questo studio evidenzia come il trattamento con Ozonoterapia si sia rivelato efficace sia nel controllo del dolore sia nella riduzione dell’edema osseo
Key words
Epicondylitis, pain, bone oedema, ozone therapy, efficacy
Parole chiave
Epicondilite, dolore, edema osseo, ozonoterapia, efficaciaIntroduction
Epicondylitis is a condition that primarily affects the short radial extensor muscle of the carpus at its bony insertion on the humeral epicondyle. This condition usually has a microtraumatic degenerative cause and causes severe local, often chronic pain, associated with difficulty in performing certain specific movements.1
In common clinical practice, it is most frequently found in people who perform work and/or sports activities, or even in those who do not perform particularly heavy occupations. It is important to remember, in fact, that the affected muscle is stressed during any movement of the wrist and hand, even the simplest and most repetitive, such as writing, typing on a keyboard, turning a key or driving.
The age group most affected is between 30 and 50.
The patient's examination and reported complaints are usually strongly indicative of the condition. Epicondyle pain on wrist extension, pain on palpation of the epicondyle, the Mills test (passive wrist flexion) and the Cotzen test (active resisted wrist extension) are all obvious signs of such inflammation.
Bone oedema is an inflammatory process that occurs within the trabecular or spongy bone. It can be caused by trauma or degenerative diseases such as arthritis, osteoarthritis and osteoporosis.2
Bone oedema can be caused by the bone's response to overexertion. This causes damage to the solid tissues, such as calcium, phosphorus and collagen fibres, which can no longer provide stability and flexibility to the body because they are worn out.
Materials and methods
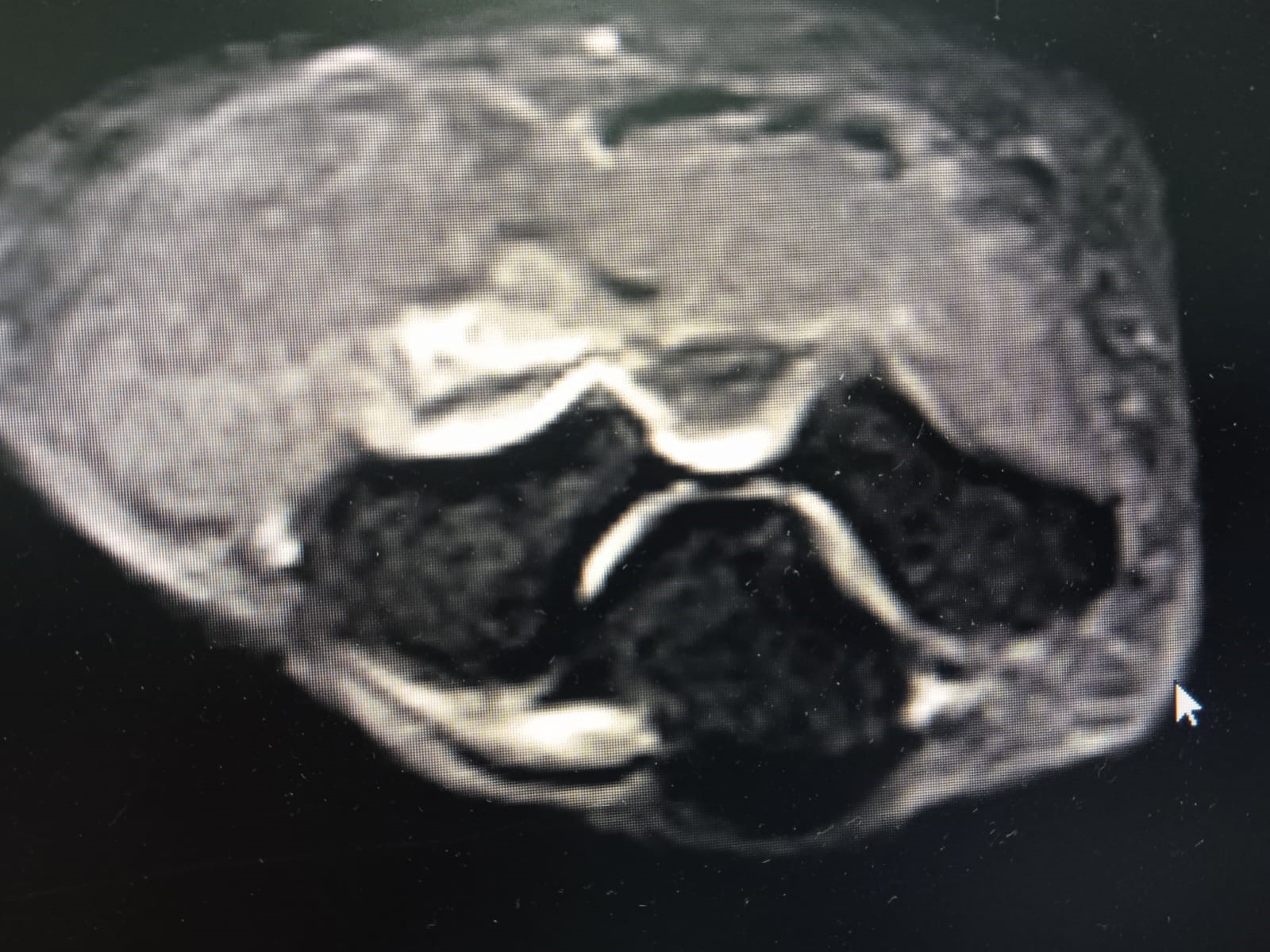
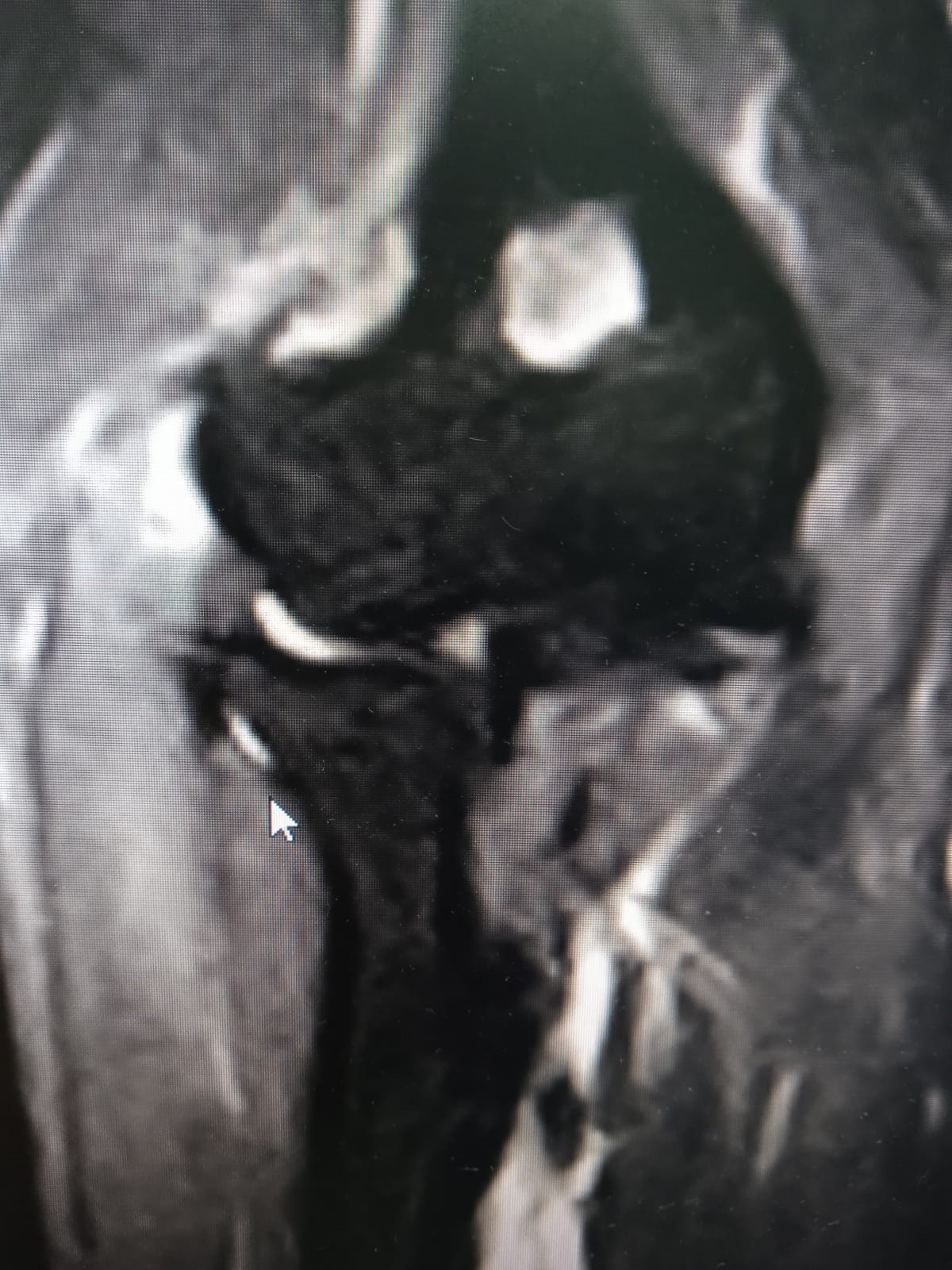
A 48-year-old man suffering from epicondylitis for about 6 months following a sports injury comes to our outpatient pain therapy clinic. On an MRI scan in January 2024 (Figures 1 and 2), he presented with extensive bone oedema. The patient complains of pain of 10 in the anterolateral region of the right elbow (assessed with the NRS numeric scale) and functional impotence in prone-supination movements of the forearm.
The patient underwent 10 injections near the extensor tendons of the fingers at the level of the right elbow under ultrasound guidance at our pain therapy clinic performed sterilely on a weekly basis with a mixture of Oxygen-Ozone at 15 μg/ml.
Trattamenti pregressi
The patient had already undergone physiotherapy treatments with weekly sessions of 20 T.E.C.A.R. therapy and 20 laser therapy, then 12 sessions of shock waves, he also placed a specific brace for 60 days without any benefit.
He took Diclofenac 150 mg c, 2 tablets per day in 10-day cycles per month for 3 months, alternating with acetaminophen and codeine formulations (500 mg acetaminophen and 30 mg codeine), 1 tablet every 8 hours for 15 days.
These treatments reduced pain by 20% (NRS 8), but without improving joint motility.
Ozone therapy
Previous treatments had only partially reduced the pain (NRS numeric scale 10 to 8) but no improvement in elbow joint function or forearm movement had been noted.
The patient came to our Centre, where he underwent ultrasound-guided injections of ozone (15%) volume 20 ml, weekly for 8 sessions in total.
The mixture of oxygen and ozone was injected under ultrasound guidance near the extensor tendons of the fingers.
Results
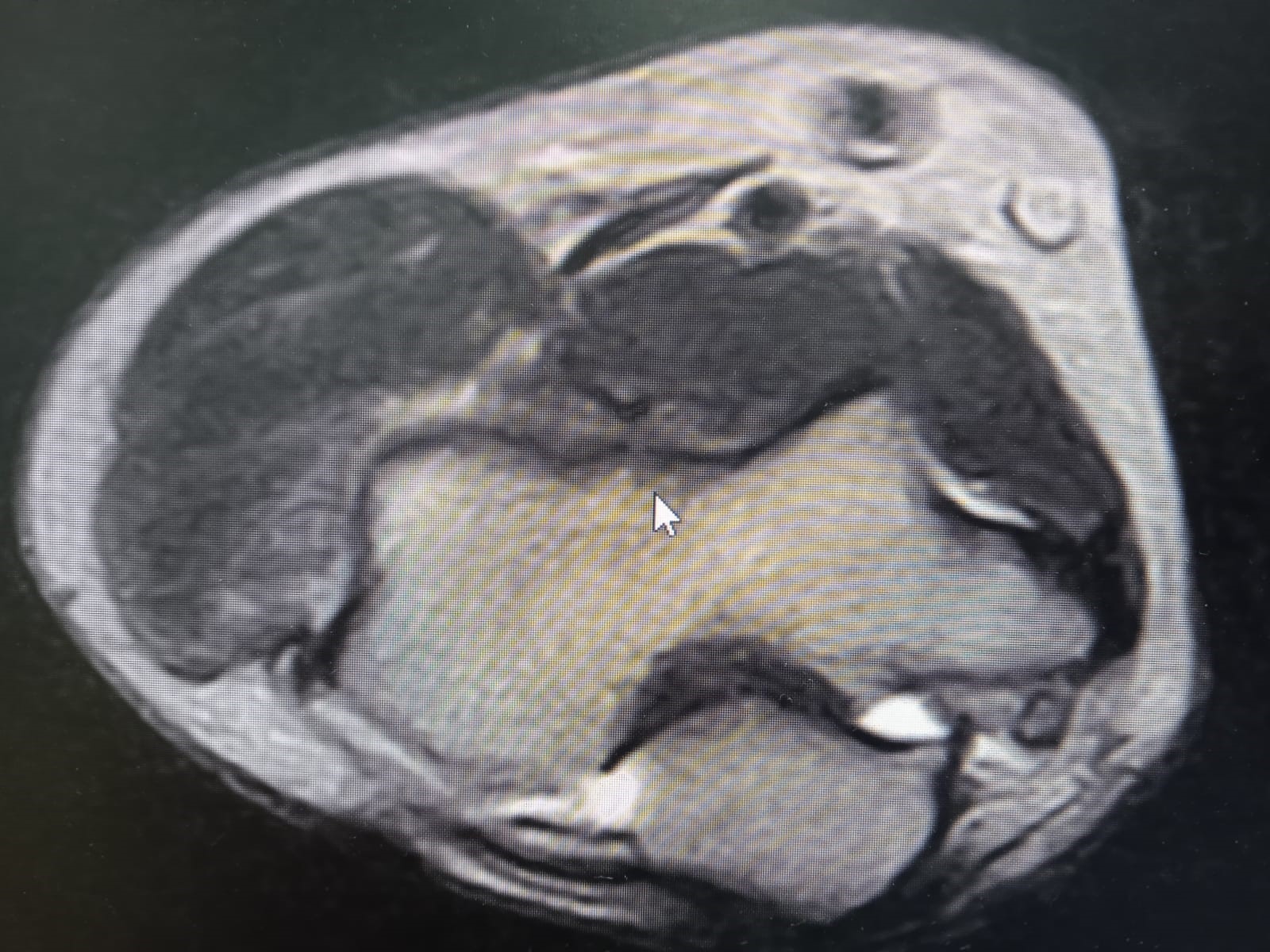
The ultrasound scan after the first four sessions showed a 40% reduction in bone oedema and a 50% reduction in pain. Given the encouraging results, we continued the treatment with a further four ultrasound-guided ozone injections, by the end of which the pain had disappeared. At the end of the treatment, the patient reported 0 pain on the NRS numerical scale. Only mild discomfort and discomfort with some forearm abduction movements remained.
The bone oedema was reduced, as can be seen from the MRI scans taken before (Figure 1 and Figure 2) and after the ozone therapy treatment (Figure 3 and Figure 4).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Discussion
The administration of ozone has many beneficial effects on our organism.3 Specifically, it stimulates the release of endorphins, substances that inhibit the transmission of harmful signals; it has an anti-inflammatory effect, increasing anti-inflammatory cytokines and reducing pro-inflammatory cytokines. It has an analgesic action, which is important in terms of muscle relaxation, vasodilation and reactivation of muscle metabolism. Ozone increases the synthesis of adenosine triphosphate (ATP), the energy reserve of cells, which causes calcium reabsorption and consequently, oedema.4
O2/O3 infiltrations are becoming increasingly popular for the treatment of musculoskeletal disorders. Since the 1990s, this procedure has also been used to treat acute and chronic polyarthritis (hip, knee, sacroiliac and interphalangeal joints), tendonitis, epicondylitis, carpal tunnel syndrome and myofascial pain.5,6
Several authors have described the anti-inflammatory, analgesic and anti-oedema properties of injected medical ozone, suggesting and proposing that the oxidation of algogenic receptors would inhibit the pain signal and activate the antinociceptive system.7,8,9
In our clinical case, the mixture of oxygen and ozone, administered at a concentration of 15 μg/ml (20 ml volume) via the peritendinous ultrasound route, effectively reduced bone oedema and pain.
Conclusion
Il presente caso clinico dimostra che l'utilizzo della miscela ossigeno ozono è utile nel riassorbimento dell'edema osseo e del dolore nell'epicondilite.
Conflict of interest
Gli autori dichiarano assenza di conflitto di interessi
Open Access-license (CC BY-NC 4.0)
Read Non-Commercial license
Published
15th November 2024
References
1. Ahmed AF, Rayyan R, Zikria BA, Salameh M.Lateral Epicondylitis of the elbow: an up-to-date review of management.Eur J Orthop Surg Traumatol. 2023 Feb;33(2):201-206
2. Eustace S, Keogh C, Blake M, Ward RJ, Oder PD, Dimasi M. MR imaging of bone oedema: mechanisms and interpretation. Clin Radiol. 2001 Jan;56(1):4-12.
3. Velio Alvaro Bocci. Scientific and medical aspects of ozone therapy. State of the art. Arch Med Res 2006;37 (4):425-35. doi: 10.1016/ j.arcmed. 2005.08.006.
4. Madej P, Antoszewski Z, Madej JA. Ozonotherapy. Mater Med Pol. 1995 Apr-Jun;27(2):53-6.
5. Gökhan Ragip Ulusoy, Ali Bilge, Ömür Öztürk Comparison of corticosteroid injection and ozone injection for relief of pain in chronic lateral epicondylitis Acta Orthop Belg - 2019 Sep;85(3):317-324.
6. Zakharash MP, Malynovs'kyĭ Siu. Use of ozonotherapy in clinical practice. Lik Sprava. 2005 Jul-Sep;(5-6):10-7.
7. De Sire A, Agostini F, Lippi L, Mangone M, Marchese S, Cisari C, Bernetti A, Invernizzi M. Oxygen-Ozone Therapy in the Rehabilitation Field: State of the Art on Mechanisms of Action, Safety and Effectiveness in Patients with Musculoskeletal Disorders. Biomolecules. 2021 Feb 26;11(3):356. doi: 10.3390/biom11030356.
8. Liao CD, Chen HC, Huang MH, Liou TH, Lin CL, Huang SW. Comparative Efficacy of Intra-Articular Injection, Physical Therapy, and Combined Treatments on Pain, Function, and Sarcopenia Indices in Knee Osteoarthritis: A Network Meta-Analysis of Randomized Controlled Trials. Int J Mol Sci. 2023 Mar 23;24(7):6078. doi: 10.3390/ijms24076078.
9. Raeissadat SA, Ghazi Hosseini P, Bahrami MH, Salman Roghani R, Fathi M, Gharooee Ahangar A, Darvish M. The comparison effects of intra-articular injection of Platelet Rich Plasma (PRP), Plasma Rich in Growth Factor (PRGF), Hyaluronic Acid (HA), and ozone in knee osteoarthritis; a one year randomized clinical trial. BMC Musculoskelet Disord. 2021 Feb 3;22(1):134. doi: 10.1186/s12891-021-04017-x.