Chronic low back pain: pulsed radiofrequency treatment
Dolore lombare cronico: trattamento con radiofrequenza pulsata
Clinical report
Pathos 2020; 27, 2. Online 2020, Aug 27
_______________________________________________________________________________
Stefano Brauneis,1 Enza Sorrentino,1 Fabio Araimo,2
Martina Novelli,1 Vincenza Di Lisa,1 Giuseppe La Torre,3
Francesco Pugliese 2
1 Pain Center
2 Neurosurgery
3 Dipartimento di Sanità pubblica e Malattie infettive
Policlinico Umberto I Hospital,
“Sapienza” University of Rome (Italy)
_____________________________________________________
Summary
Chronic low back pain (CLBP) is an insidious disorder from a treatment point of view. The aim of the study was to evaluate the effectiveness of a pulsed radiofrequency treatment in association with medical therapy in LBP. 40 patients affected by CLBP, due to facet and/or sacroiliac joint dysfunction, were enrolled. A pulsed radiofrequency (PRF) treatment was performed in association with medical therapy. The evaluation of NRS, DN4 and Roland Morris Disability Questionnaire (RMDQ) was made in a first visit and in a second visit after the treatment. The control group (100 patients) was treated with a medical therapy only. Comparing the values of NRS between V0 and V1 the reduction was more consistent in the treatment group compared to the control group. Even the values of DN4 and RMDQ were found to be lower than V1 compared to V0, in the treatment group than in the control group. The preliminary results show that a PRF treatment associated to a medical therapy seems to be more effective than just the medical therapy in CLBP treatment.
Riassunto
Il dolore lombare cronico (CLBP) è un disturbo insidioso da trattare. Lo scopo dello studio è valutare l’efficacia di un trattamento di radiofrequenza pulsata (PRF) in associazione alla terapia medica, nel LBP. Sono stati arruolati 40 pazienti affetti da LBP dovuto a sindrome faccettale e/o disfunzione dell’articolazione sacro-iliaca. In associazione alla terapia medica è stato effettuato un trattamento di PRF. Sono stati valutati i valori di NRS, DN4 e Roland Morris Disability Questionnaire (RMDQ), sia in una prima visita sia in una successiva post-trattamento.
Il gruppo di controllo (100 pazienti) è stato trattato con la sola terapia medica. Comparando i valori di NRS tra V0 e V1, la riduzione è stata più consistente nel gruppo di trattamento. Anche i valori di DN4 e RMDQ risultato maggiormente ridotti tra V0 e V1 nel gruppo di trattamento rispetto al gruppo di controllo. I risultati preliminari suggeriscono che un trattamento di PRF associato alla terapia medica sia più efficace della sola terapia medica.
Key words
Pulsed radiofrequency, chronic low back pain, facet syndrome, sacroiliac joint
Parole chiave
Radiofrequenza pulsata, dolore lombare cronico, sindrome faccettale, articolazione sacroiliaca
Introduction
Chronic low back pain (CLBP) is associated with several underlying diseases that include conditions not suitable of surgical treatment like facet joints, sacroiliac joints dysfunction, etc.1,2 Facet joints is source of pain in 15% of case of chronic low back pain.3 Sacroiliac joint dysfunction affected 10-25% of patients with low back pain.4 In these patients, therapeutic options rely on staircase increasing multimodal treatment that include physical rehabilitation, pharmacological and physical therapies.5,6 The use of minimally invasive therapies as local infiltration, medial branch neurotomy, epidural injection, pulsed radiofrequency (PRF), are also possible as second tier approach in the multimodal treatment.7,8
The PRF has been used for the treatment of various pain syndromes, with positive clinical effects in trigeminal neuralgia, occipital neuralgia, shoulder pain, pubalgia, knee osteoartrithis, ankle pain.9-12 This technique is based on direct application of an electro-magnetic field on sensory fibres and the related biological and neuromodulators effects, with apparent lack of side effects.13,14 Despite the wide use of pulsed radiofrequency in the treatment of chronic low back pain, data on efficacy are conflicting. This prospective non randomized clinical trial is intended to evaluate the effects of including PRF to a multimodal therapeutic strategy in the symptomatic treatment of patients with chronic low back pain due to facet syndrome or sacroiliac joint dysfunction in terms of pain severity and functional status.
Materials and methods
Patients
40 patients with CLBP caused by facet syndrome and/or by sacroiliac joint dysfunction were enrolled at Pain Center of the Umberto I Hospital in Rome. All patients expressed informed consent. Our ethical committee approved the study.
Inclusion criteria
Patients of both sexes, aged between 18 and 80, were included in the study with Numerical rating scale value (NRS) =6 on the first examination, diagnosed with facet syndrome or sacroiliac dysfunction confirmed by positive diagnostic blockage performed under fluoroscopic guidance.
Exclusion criteria
Patients with PMK, with allergies to local anaesthetics, coagulopathies or previous undergoing radiofrequency treatment for the same pathology, were excluded from the study.
Methods
All patients underwent a first medical exam (V0): anamnestic data, instrumental and blood chemistry test reports, NRS, “Neuropathic pain four questions” (DN4) and “Roland Morris Disability Questionnaire” (RMDQ) were collected. All patients were prescribed medical therapy on WHO scale, (acetaminophen, Fans, adjuvants and weak opioids based on pain level). Patients were then subjected to a fluoroscopic-guided diagnostic block, 50% pain relief was diagnostic in facet syndrome15 and 75% in the dysfunctions of the sacroiliac joint.16,17
A pulsed radiofrequency treatment was performed one week after the diagnostic block in the angiographic room under fluoroscopic TC cone beam guidance. In patients with facet syndrome, treatment was performed on the medial branches of the vertebral level corresponding to the pain and upper vertebral level.18 In patients with sacroiliac joint dysfunction treatment was performed on the medial branch of the L5-S1 joint and on the lateral sacral branch at the level of the first and the second sacral foramen.19,20 In both cases, the points were identified by needle 22G 100 mm, after the recording of values of impedance, execution of sensitive stimulation and control motor stimulation, 600 pulses were given at 45 Volt with maximum temperature reached 42° C for each point, in pulsed mode. NRS, DN4 and RMDQ values were collected during a second visit (V1), two months after the first one. The control group included 100 patients who were treated in the same centre between January 2016 and September 2018, for the same condition with medical therapy only, prescribed according to OMS scale. Mann-Whitney’s test and Wilcoxon signed-rank test were performed for the analysis of nonparametric variables and Fisher’s test was performed for dichotomic variables.
A pulsed radiofrequency treatment was performed one week after the diagnostic block in the angiographic room under fluoroscopic TC cone beam guidance. In patients with facet syndrome, treatment was performed on the medial branches of the vertebral level corresponding to the pain and upper vertebral level.18 In patients with sacroiliac joint dysfunction treatment was performed on the medial branch of the L5-S1 joint and on the lateral sacral branch at the level of the first and the second sacral foramen.19,20 In both cases, the points were identified by needle 22G 100 mm, after the recording of values of impedance, execution of sensitive stimulation and control motor stimulation, 600 pulses were given at 45 Volt with maximum temperature reached 42° C for each point, in pulsed mode. NRS, DN4 and RMDQ values were collected during a second visit (V1), two months after the first one. The control group included 100 patients who were treated in the same centre between January 2016 and September 2018, for the same condition with medical therapy only, prescribed according to OMS scale. Mann-Whitney’s test and Wilcoxon signed-rank test were performed for the analysis of nonparametric variables and Fisher’s test was performed for dichotomic variables.
A p value<0,05 was considered as statistically significant. Statistical data were analyzed through the statistical software SPSS 25.
Preliminary results
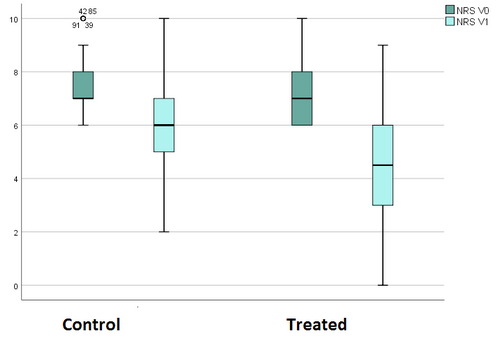
A total of 140 patients were included in the study, 40 in the treatment group and 100 in the control group. The two groups have similar characteristics in terms of age, sex and type of pain. Patients in the treatment group had 7.38 ± 1.295 NRS values at V0. Patients in the control group had NRS values of 7.46 ±1.15 at V0. Patients in the treatment group recorded 4.5 ± 2.08 NRS values at V1, with a mean NRS delta of -2.87 ±1.6. Patients in the control group had NRS values at V1 of 5.65 ±1.54, with a mean NRS delta of -1.81 ± 1,27 (p<0,005) (Figure 1).
{kind=link}
We had DN4 values of 2.46 ± 1.86 for V0 and 1.56 ± 1.53 for V1 in total in the 140 patients studied. There was then a delta DN4 between V0 and V1 of -0,73± 0,8 in the control group and a delta DN4 between V0 and V1 equal to –1,32± 1,1 in the treated group (p<0,005) (Figure 2).
{kind=link}
The two groups, control and treated were homogeneous by degree of disability assessed with Roland Morris Disability Questionnaire. We recorded a Delta RMDQ between V0 and V1 in the control group equal to –1.87± 1.44 and a Delta RMDQ in the treated group equal to –2.3± 2.4 (p<0,005) (Figure 3).
{kind=link}
Discussion
Pain relief obtained with pulsed radiofrequency in chronic low back pain varies from 3 to 16 months in low back pain associated with facet syndrome21-25 and from 6 to 12 months in low back pain with sacroiliac joint involvement.26-28 The aim of this study was to assess the effectiveness of pulsed radiofrequency in combination with medical therapy. The level of pain was assessed with NRS value. The results showed a reduction of NRS value from V0 to V1 around 39% in the treatment group (mean reduction of 2.87 points of NRS) and around 24% in the control group (mean reduction of 1,81 NRS points). The results showed a high variation from the standard value of NRS (standard deviation 1,18 to V0 and 1,7 to V1). This result could be related to psychometric characteristics of the patient (threshold of pain, cultural level, character, attitude towards pain).29 Approximately 40% of the patients in the treatment group reported a few-day increase in NRS in the days immediately following the procedure. However, not perceived as debilitating or required further pharmacological intake. At V1, patients in the treatment group reported unchanged or reduced NRS values compared to V0, in no case increased. In the control group, two patients reported unchanged values of NRS between V0 and V1, in a single case NRS value was increased from V0 to V1. This result could be justified by the side effects related to the use of drugs, which may have possibly distorted the perception of effectiveness of the medical therapy. Side effects such as dizziness, drowsiness, and nausea have been reported by patients taking gabapentinoids pharmacological adjuvants to treat the neuropathic component, and those patients who have taken weak opioids.
The neuropathic component was evaluated with a DN4 questionnaire. This component was not present in all patients (score DN4 = 0), this to indicate that the involvement of the articular facets and the sacroiliac joint are not necessarily related to neuropathic pain. In patients with a non-zero score, the DN4 has been subject to small variations, more consistent in the treated group than in the control group (mean delta DN4 equal to -1,32 points in the treated group, -0,7 points in the control group). Three patients with DN4>0 at V0 in the treatment group had unchanged values at V1. In the control group, 13 patients reporting DN4>0 reported unchanged values to V1. No patients had increased values of DN4 to V1, either in the treatment group or in the control group. From the data extracted from the Roland Morris Disability Questionnaire, both the facet syndrome and the dysfunctions of the sacro-iliac articulation seem to affect the degree of disability. The questionnaire investigates aspects of everyday life, on which low back pain can burden lowering the quality of life: 15 questions are related to the physical category, 3 to sleep and rest, 2 to the psychosocial sphere, 2 to domestic management and 1 to appetite and 1 to frequency of pain. The patient is asked to refer to the situation at that time. The phrase “because of my back pain…” placed at the beginning of each point only allows to investigate LBP as a cause of disability and the exclusion of other causes of disability. Both groups settle on RMDQ values at V0 around 15 out of a total of 24 questions, thus presenting, at the time of the first visit, a moderate-severe degree of disability. In the treatment group the reduction in this score was about 2.3 points higher than 1.87 in the control group. In 5 of the patients in the treatment group, RMDQ values between V0 and V1 did not change, in no case increased RMDQ values were detected. In 17 patients in the control group RMDQ values did not change between V0 and V1, no increased values were found. Many authors concluded that RMDQ is more sensitive in detecting changes in functional limitation than other tests30-32 The changes in score identified in the study groups well correlate with an improvement in the degree of disability.
An observation is required on the method of execution of the procedures. The use of the TC cone beam fluoroscope allowed for greater precision of the procedure. In case of doubts in the anteroposterior or lateral projections, it was possible to quickly perform CT scans and 3D reconstructions with excellent spatial and contrast graphic reconstruction, which have optimized the visualization of the target structures and the position of the electrode-needle, without burdening the patient with X-ray absorption; This technology is designed to minimize the emission of x-rays, for greater safety of both the patient and the health care staff.33-35
The results obtained showed that PRF treated patients had a best outcome in terms of pain level, reduction of the neuropathic component, where present, and disability reduction, than the control group. No side effects have been reported in the treatment group, no complications during the procedure were detected. The only relevant finding in terms of adverse effects was the momentary increase in NRS reported by approximately 40% of patients in the treatment group that only lasted a few days and did not require a rescue therapy.
Conclusion
From the preliminary results obtained, the treatment of PRF in low back pain with involvement of the articular facets or sacroiliac joint, seems to be effective. The PFR could be considered as a strategy to reduce patient drug use and disability, given its few or no side effects, the possibility to repeat the treatment at the end of the effects and few contraindications. The optimization of the method of execution and the careful selection of patients, allows a greater chance of success of the treatment, greater safety and satisfaction for the patient.
Conflict of interests
The authors certify the study was conducted without conflict of interests.
Published
27th August 2020
Correspondence
stefano.brauneis@uniroma1.it
References
1) Tavee JO et al. Low Back Pain. Continuum 2017; 23(2): 467-486.
2) Juch JNS et al. Effect of Radiofrequency Denervation on Pain Intensity Among Patients With Chronic Low Back Pain: The Mint Randomized Clinical Trials. JAMA 2017; 318(1): 68-81.
3) Cohen SP et al. Pathogenesis, Diagnosis, and Treatment of Lumbar Zygapophysial (Facet) Joint Pain. Anesthesiology 2007; 106: 591-614.
4) Hansen H et al. A Systematic Evaluation of the Therapeutic Effectiveness of Sacroiliac Joint Interventions. Pain Physician 2012; 15(3): E247-78.
5) Qaseem A et al. Noninvasive Treatments for Acute, Subacute, and Chronic Low Back Pain: A Clinical Practice Guideline From the American College of Physicians. Ann Intern Med 2017; 166 (7): 514-530.
6) Oliveira CB et al. Clinical practice guidelines for the management of non-specific low back pain in primary care: an updated overview. European Spine Journal 2018; 27: 2791-2803.
7) Chou R et al. Nonsurgical interventional therapies for low back pain: a review of the evidence for an American Pain Society clinical practice guideline. Spine (PhilaPa) 2009; 34 (10): 1078-93.
8) Koes BW et al. Diagnosis and treatment of low back pain. BMJ 2006; 332:1430-34.
9) Vanneste T et al. Pulsed radiofrequency in chronic pain. Curr Opin Anesthesiol 2017; 30.
10) Masala S et al. Pulse-dose radiofrequency for knee osteoartrithis. Cardiovasc Intervent Radiol 2014; 37(2):482-7.
11) Masala S et al. Pulse-Dose Radiofrequency in Athletic Pubalgia: Preliminary Results. J Sport Rehabil 2017; 26(3): 227-233.
12) Facchini G et al. A comprehensive review of pulsed radiofrequency in the treatment of pain associated with different spinal conditions. Br J Radiol 2017;90(1073):20150406.
13) Bogduk N. Pulsed radiofrequency. Pain Med 2006; 7(5): 396-407.
14) Vallejo R et al. Pulsed radiofrequency modulates pain regulatory gene expression along the nociceptive pathway. Pain Physician 2013; 16(5): E601-13.
15) Cohen SP et al. Establishing an optimal "cutoff" threshold for diagnostic lumbar facet blocks: a prospective correlational study. Clin J Pain. 2013 May;29(5): 382-91.
16) Vleeming A et al. The sacroiliac joint: an overview of its anatomy, function and potential clinical implications. J Anat 2012; 221(6): 537-67.
17) Zlomislic V et al. Management of Sacroiliac Joint Dysfunction. Contemporary Spine Surgery 2012 Mar; Volume 13, Number 3.
19) Patel N et al. A Randomized, Placebo-Controlled Study to Assess the Efficacy of Lateral Branch Neurotomy for Chronic Sacroiliac Joint Pain Medicine 2012; 13: 383-398.
20) Soto Quijano DA et al. Sacroiliac Joint Interventions. Phys Med Rehabil Clin N Am 2018; 29(1): 171-183.
21) Nath S et al. Percutaneous lumbar zygapophysial (Facet) joint neurotomy using radiofrequency current, in the management of chronic low back pain: a randomized doubleblind trial. Spine (Phila Pa 1976) 2008; 33(12):1291-7.
22) Kim DH et al. Efficacy of pulsed radiofrequency medial branch treatment in low back pain patients. J Back Musculoskelet Rehabil. 2016; 29(2): 361-366.
23) Chua NHL et al. Pulsed radiofrequency treatment in interventional pain management: mechanisms and potential indications-a review. Acta Neurochir (Wien) 2011;153(4): 763-71.
24) Lindquist J et al. Pulsed radiofrequency in clinical practice. A retrospective analysis of 238 patients with chronic noncancer pain treated at an academic tertiary pain centre. Scand J Pain 2016; 12: 68-73.
25) Chang MC et al. Intraarticular Pulsed Radiofrequency to Treat Refractory Lumbar Facet Joint Pain in Patients with Low Back Pain. World Neurosurg 2018;112: e140-e144.
26) Yuanyuan D et al. Clinical observation of CT-guided intraarticular conventional radiofrequency and pulsed radiofrequency in the treatment of chronic sacrumiliac joint pain J Pain Res 2018; 11: 2359-2366
27) Dutta K et al. Comparison of Efficacy of Lateral Branch Pulsed Radiofrequency Denervation and Intraarticular Depot Methylprednisolone Injection for sacroiliac joint pain. Pain Physician 2018; 21(5): 489-496.
28) Chang MC et al. The effect of intra-articular stimulation by pulsed radiofrequency on chronic sacrumiliac joint pain refractory to intra-articular corticosteroid injection: a retrospective study. Medicine (Baltimore) 2017; 96(26): e7367.
29) Rating Scales, Verbal Rating Scales, and Visual Analogue Scales for assessment of pain intensity in adults: a systematic literature review. J Pain Symptom Manage 2011; 41(6): 1073-93.
30) Grotle M et al. Functional status and disability questionnaires: what do they assess? A systematic review of backspecific outcome questionnaires. Spine (Phila Pa 1976) 2005;30:130-40.
31) Grotle M et al. Concurrent comparison of responsiveness in pain and functional status measurements used for patients with low back pain. Spine (Phila Pa 1976) 2004;29: E492-501.
32) Smeets R et al. Measures of Function in Low Back Pain/Disorders. Arthritis Care & Research 2011; 63 (S11): S158-S173.
33) Michael F et al. Fluoroscopic Cone Beam CT for Guidance of Minimally Invasive Spine Interventions. Pain Physician 2010; 13:51-59.
34) Santhosh R et al. Carm Cone Beam Computed Tomography: A New Tool in the Interventional Suite. Ann Acad Med Singapore 2013; 42:585-92.
35) Dajie Wang. Image Guidance Technologies for Interventional Pain Procedures: Ultrasound, Fluoroscopy, and CT. Current Pain and Headache Reports 2018; 22: 6.