Craniofacial pain and high frequency stimulation
Dolore cranio faciale e neurostimolazione ad alta frequenza
Casi clinici
Pathos 2016; 23; 2. Online 2016, Sep 6
____________________________________________________________________
Alfonso Papa, Maria Teresa Di Dato, Pietro Buonavolontà,
Dario Tammaro, Andrea Pironti, Elisabetta Saracco, Maurizio Ferrara, Antonio Corcione
Dipartimento Area Critica- UOSD Terapia del Dolore AO dei Colli-V. Monaldi, Napoli
_____________________________________________________________________
Summary Neuromodulation is a treatment modality that shows promise and so far case reports have used peripheral approaches to the trigeminal ganglion and its branches. We describe the use of high frequency spinal cord stimulation at the cervical spine as a novel approach to management of refractory trigeminal neuralgia.
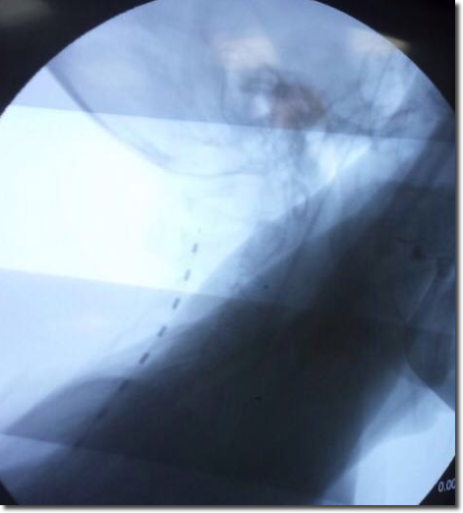
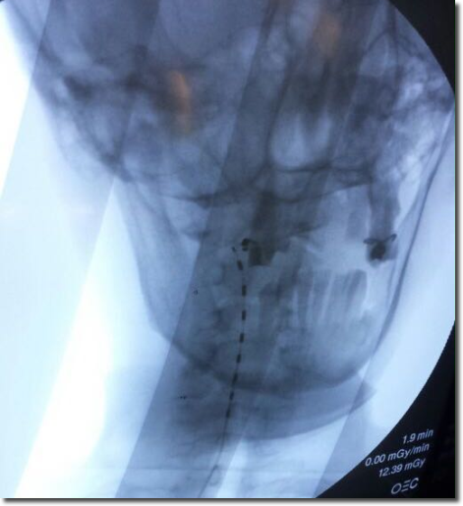
We have enrolled 3 patients, suffering from trigeminal neuralgia involving the first branch of nerve. All the patients had been implanted with one octopolar electrode such that the stimulating contacts were placed at the C2-C3 vertebral level; electrodes had been connected to an external trial lead extension, which was removed at the end of the trial with subsequent implantation of the definitive IPG.
All the patients completed trial period with successful implantation because pain relief was about 70%. All the patients decreased analgesics consumption, especially for opioids.The application of electrical pulses directly onto the dorsal columns at the C2-C3 vertebral level provide a neuromodulatory effect on the Trigemino-Cervical Complex (TCC) greater than peripheral trigeminal branches stimulation.
Riassunto La neurostimolazione è un trattamento moderno ed estremamente promettente; numerosi approcci periferici sono stati sinora applicati al trigemino e alle sue branche. Di seguito si descrive la neurostimolazione midollare ad alta frequenza come tecnica moderna di approccio al trattamento della nevralgia del trigemino refrattaria.
Abbiamo arruolato 3 pazienti, affetti da nevralgia della prima branca del nervo. Tutti i pazienti sono stati sottoposti ad impianto di un elettrodo ottopolare con posizionamento dei contatti stimolanti a livello vertebrale C2-C3; gli elettrodi sono stati connessi ad un’ estensione esterna di prova, rimossa alla fine del periodo di prova con conseguente impianto dell’IPG definitivo.
Tutti i pazienti hanno completato il periodo di prova con impianto definitivo, per riduzione del dolore di circa il 70%. Tutti i pazienti hanno ridotto il consumo di analgesici, soprattutto oppioidi. L’applicazione di impulsi elettrici direttamente a livello della colonna dorsale, a C2-C3, esplica un effetto di neuro modulazione sul Complesso Trigemino-Cervicale (TCC) maggiore della stimolazione periferica delle branche del trigemino.
Key words Chronic pain, Neuromodulation, High Frequency Stimulation, Trigeminal Neuralgia, trigemino-cervical complex (TCC)
Parole chiave Dolore cronico, Neuromodulazione, Stimolazione ad Alta Frequenza, Nevralgia Trigeminale, Nucleo trigemino-cervicale (TCC)
Introduction
Craniofacial pain, including trigeminal neuralgia, trigeminal neuropathic pain, and persistent idiopathic facial pain, is difficult to treat and can have severe implications for suffering in patients afflicted with these conditions. In recent years, clinicians have moved beyond treating solely with pharmacological therapies, which are generally not very effective, and focused on new interventional pain procedures.1-3
Medical treatment of patients with trigeminal neuralgia is challenging as such as serious side effects frequently complicate the treatment. There are few options to treat trigeminal neuralgia once medical, surgical and mini-invasive approaches (such as PENS and radiofrequency) have failed.4,5
Neuromodulation is a treatment modality that shows promise and so far case reports have used peripheral approaches to the trigeminal ganglion and its branches.6-9 We describe the use of high frequency spinal cord stimulation at the cervical spine as a novel approach to management of refractory trigeminal neuralgia.10,11
Materials and methods
We have enrolled 3 patients, suffering from trigeminal neuralgia involving the first branch of nerve. All the patients completed baseline pain assessment by the Numeric Rating Scale.12,13
Initially, we treated them with oral pharmacological therapy, with non-invasive technique such as PENS, and with subcutaneous stimulation with quadripolar electrodes, without clinical effect and with one explantation due to cutaneous dehiscence. Finally , we enrolled them for a trial of SCS at cervical level. All the patients had been implanted with one octopolar electrode such that the stimulating contacts were placed at the C2-C3 vertebral level; electrodes had been connected to an external trial lead extension, which was removed at the end of the trial with subsequent implantation of the definitive IPG. At the end of the trial period (15 days) of high frequency stimulation, we evaluated reduction of pain intensity and decrease of analgesics consumption too in order to enroll the patients to IPG implantation. Follow-up was established at 3 and 6 months.1
Discussion
All the patients completed trial period with successful implantation because pain relief was about 70 per cent. No adverse events had been observed; just one patient experienced prolonged postoperative pain, treated with antinflammatory drugs. All the patients decreased analgesics consumption, especially for opioids; they all had been treated with tapentadolo from 100 to 250 mg/day, reduced for two patients to 50 mg/day and stopped for the third one.
Conclusion
The application of electrical pulses directly onto the dorsal columns at the C2-C3 vertebral level provide a neuromodulatory effect on the Trigemino-Cervical Complex (TCC) greater than peripheral trigeminal branches stimulation. Cervico-medullary spinal cord stimulation has been used for the last 30 years to treat head and facial pain non-responsive to other options, but it requires expensive costs, time consuming and complex surgical procedures.1,3
Different stimulation frequencies are now available (burst stimulation, 10kHz high frequency stimulation8,9 in SCS. Those provide a new alternative to peripheral (low-frequency) stimulation due to their ability to achieve pain relief without causing any perceived sensation but its efficacy and potential side effects are unknown. Future randomized control trials of SCS in chronic, refractory headaches are still in course,1,2 and probably something new about pathophysiology will be acquired during next years.
Conflict of interest
The authors certify the study was conducted without conflicts of interest.
Published
6th Septemper 2016
Correspondence
marisita@libero.it
References
1) Al-Kaisy A, Pang D, Fenech C. High frequency cervical spinal cord stimulation in the treatment of refractory trigeminal neuralgia; Pain Management and Neuromodulation Centre, St Thomas’ Hospital, Westminster Bridge Road, London, UK.
5) Steiner TJ, Antonaci F, Jensen R, Lainez MJ, Lanteri-Minet M, Valade D. European Headache Federation, Global Campaign against Headache. Recommendations for headache service organisation and delivery in Europe. J Headache and Pain 2011; 12: 419–426.
6) Pedersen JL, Barloese M, Jensen RH. Neurostimulation in cluster headache: A review of current progress. Cephalalgia 2013; 2013 Oct;33(14):1179-93. doi: 10.1177/0333102413489040.
7) Reed KL, Black SB, Banta CJ 2nd, Will KR. Combined occipital and supraorbital neurostimulation for the treatment of chronic migraine headaches: initial experience. Cephalalgia 2010; 30:260–71.
8) Barolat G, Ketcik B, He J. Long-term outcome of spinal cord stimulation for chronic pain management. Neuromodulation 1998; 1: 19–29.
9) Bartsch T, Goadsby PJ. Stimulation of the greater occipital nerve induces increased central excitability of dural afferent input. Brain 2002; 125, 1496–1509.
10) Al-Kaisy A, Van Buyten JP, Smet I, Palmisani S, Pang D, Smith T. Sustained effectiveness of 10 kHz high-frequency spinal cord stimulation for patients with chronic, low back pain: 24-month results of a prospective multicenter study. Pain Med 2014; 15, 347–354.
11) Al-Kaisy A, Palmisani S, Smith T, Harris S, Pang D. The use of 10-Kiloherts spinal cord stimulation in a cohort of patients with chronic neuropathic limbpain refractory to medical management. Neuromodulation 2015; 1: 18–23.
12) Bagley CL, Rendas-Baum R, Maglinte GA, Yang M, Varon SF, Lee J, Kosinski M. Validating migraine-specific quality of life Questionnaire v2.1 in episodic and chronic migraine. Headache 2012; 52: 409–421.